RamPrakash Rajalakshmi, Lingam Lakshmi
Loyola Institute of Business Administration, Loyola College Campus, Nungambakkam, Chennai, 600034, Tamil Nadu, India.
Tata Institute of Social Sciences, V.N. Purav Marg, Deonar, Mumbai, 400088, India.
BMC Public Health. 2021 Feb 12;21(1):350. doi: 10.1186/s12889-021-10352-4.
The continuing impetus for universal health coverage has given rise to publicly funded health insurance schemes in lower-middle income countries. However, there is insufficient understanding of how universal health coverage schemes impact gender equality and equity. This paper attempts to understand why utilization of a publicly funded health insurance scheme has been found to be lower among women compared to men in a southern Indian state. It aims to identify the gender barriers across various social institutions that thwart the policy objectives of providing financial protection and improved access to inpatient care for women.
A qualitative study on the Chief Minister's Comprehensive Health Insurance Scheme was carried out in urban and rural impoverished localities in Tamil Nadu, a southern state in India. Thirty-three women and 16 men who had a recent history of hospitalization and 14 stakeholders were purposefully interviewed. Transcribed interviews were content analyzed based on Naila Kabeer's Social Relations Framework using gender as an analytical category.
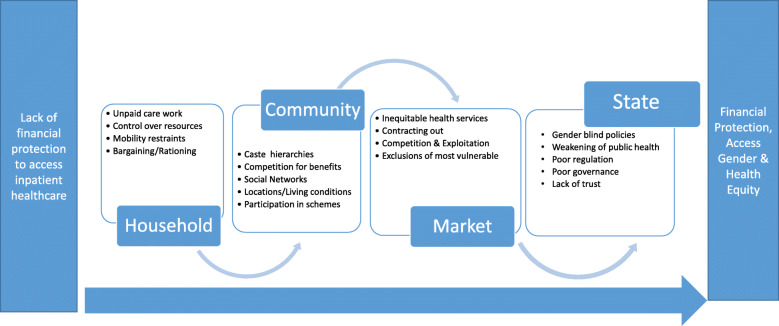
While unpacking the navigation pathways of women to utilize publicly funded health insurance to access inpatient care, gender barriers are found operating at the household, community, and programmatic levels. Unpaid care work, financial dependence, mobility constraints, and gender norms emerged as the major gender-specific barriers arising from the household. Exclusions from insurance enrollment activities at the community level were mediated by a variety of social inequities. Market ideologies in insurance and health, combined with poor governance by State, resulted in out-of-pocket health expenditures, acute information asymmetry, selective availability of care, and poor acceptability. These gender barriers were found to be mediated by all four institutions-household, community, market, and State-resulting in lower utilization of the scheme by women.
Health policies which aim to provide financial protection and improve access to healthcare services need to address gender as a crucial social determinant. A gender-blind health insurance can not only leave many pre-existing gender barriers unaddressed but also accentuate others. This paper stresses that universal health coverage policy and programs need to have an explicit focus on gender and other social determinants to promote access and equity.
全民健康覆盖的持续推动促使中低收入国家出现了公共资助的医疗保险计划。然而,对于全民健康覆盖计划如何影响性别平等和公平,人们的了解还不够充分。本文试图探究为何在印度南部一个邦,公共资助的医疗保险计划在女性中的利用率低于男性。其目的是找出各种社会机构中阻碍为女性提供经济保护和改善住院护理服务可及性这一政策目标实现的性别障碍。
在印度南部泰米尔纳德邦的城乡贫困地区,针对首席部长综合健康保险计划开展了一项定性研究。对33名近期有住院史的女性、16名近期有住院史的男性以及14名利益相关者进行了有目的的访谈。根据奈拉·卡比尔的社会关系框架,以性别为分析类别,对访谈记录进行了内容分析。
在剖析女性利用公共资助医疗保险获得住院护理的路径时,发现性别障碍在家庭、社区和项目层面均有存在。无酬护理工作、经济依赖、行动受限以及性别规范成为家庭层面出现的主要性别特定障碍。社区层面保险登记活动中的排斥现象是由多种社会不平等因素介导的。保险和医疗领域的市场观念,再加上国家治理不善,导致了自付医疗费用、严重的信息不对称、护理服务的选择性提供以及可接受性差。这些性别障碍被发现是由家庭、社区、市场和国家这四个机构共同介导的,导致女性对该计划的利用率较低。
旨在提供经济保护和改善医疗服务可及性的卫生政策需要将性别作为一个关键的社会决定因素来对待。忽视性别的医疗保险不仅无法解决许多既有的性别障碍,还会加剧其他障碍。本文强调,全民健康覆盖政策和计划需要明确关注性别及其他社会决定因素,以促进可及性和公平性。