Department of Optics and Optometry and Vision Science, University of Valencia, Doctor Moliner, 50, 46100, Burjassot, Spain.
Department of Psychobiology, University of Valencia, Avda. Blasco Ibañez, 13, 46010, Valencia, Spain.
BMC Ophthalmol. 2023 Sep 28;23(1):396. doi: 10.1186/s12886-023-03116-8.
To evaluate factors associated with better outcomes from optical treatment alone in amblyopic children from 3 up to 7 years.
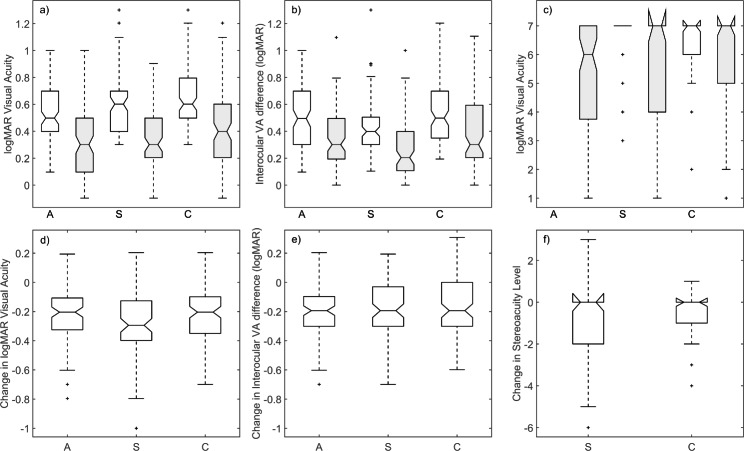
Data extracted from two studies with similar protocols, Amblyopic Treatment Studies 5 (n = 152) and 13 (n = 128) from the Pediatric Eye Disease Investigator Group database, were used to determine by regression analysis the factors associated with improvements in visual acuity in the amblyopic eye, inter-ocular visual acuity difference and stereoacuity. Input variables were aetiology of amblyopia (anisometropic, strabismic and combined-mechanism amblyopia), treatment compliance, visual acuity, interocular visual acuity difference, stereoacuity, tropia size at distance and near, age and refractive error at baseline.
Despite the range of clinical factors considered, our models explain only a modest proportion of the variance in optical treatment outcomes. The better predictors of the degree of optical treatment success in amblyopic children are visual acuity of the amblyopic eye, interocular visual acuity difference, stereoacuity, treatment compliance and the amblyopic eye spherical-equivalent refractive error. While the aetiology of the amblyopia does not exert a major influence upon treatment outcome, combined-mechanism amblyopes experience the smallest improvement in visual acuity, tropia and stereoacuity and may need longer optical treatment periods.
While results identify the factors influencing optical treatment outcome in amblyopic children, clinicians will be unable to predict accurately the benefits of optical treatment in individual patients. Whether this is because relevant clinical or non-clinical factors (e.g. nature and volume of daily activities undertaken) influences the outcomes from optical treatment has not yet been identified and remains to be discovered.
评估 3 至 7 岁弱视儿童单纯光学治疗效果较好的相关因素。
利用小儿眼病研究组数据库中两项相似方案的研究(弱视治疗研究 5 [n=152]和 13 [n=128])的数据,通过回归分析确定与弱视眼视力提高、双眼视力差异和立体视锐度相关的因素。输入变量为弱视病因(屈光不正性、斜视性和混合机制弱视)、治疗依从性、视力、双眼视力差异、立体视锐度、远距和近距斜视大小、年龄和基线时屈光不正。
尽管考虑了一系列临床因素,但我们的模型仅能解释光学治疗结果中相当小一部分的变异性。弱视儿童光学治疗成功程度的更好预测因素是弱视眼视力、双眼视力差异、立体视锐度、治疗依从性和弱视眼球镜等效屈光不正。虽然弱视的病因对治疗结果没有重大影响,但混合机制弱视患者的视力、斜视和立体视锐度改善最小,可能需要更长的光学治疗时间。
虽然结果确定了影响弱视儿童光学治疗效果的因素,但临床医生仍无法准确预测光学治疗对个别患者的益处。这是否是因为相关的临床或非临床因素(例如日常活动的性质和量)影响了光学治疗的结果仍未确定,有待发现。