Dang Huy Quang, Nguyen Cong Thanh, Pham Hoat Viet, Tran Linh Duc, Nguyen Cong Duc, Truong Dung Vu Manh, Hoang Trang Thi Kieu, Van Chau Tao
Vietnam National University Ho Chi Minh City University of Science, Ho Chi Minh City, Viet Nam.
Oncology and Nuclear Medicine, Military Hospital 175, Ho Chi Minh City, Viet Nam.
Rep Pract Oncol Radiother. 2023 Aug 28;28(4):445-453. doi: 10.5603/RPOR.a2023.0056. eCollection 2023.
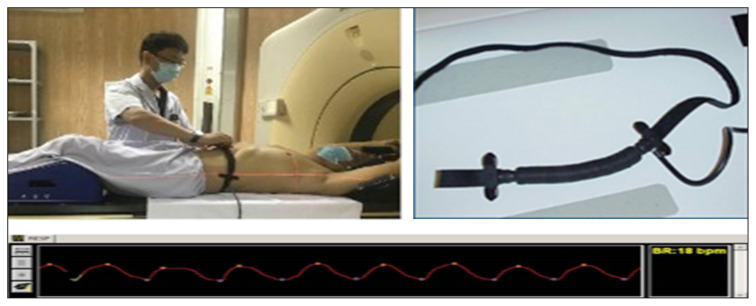
The study was to evaluate the effectiveness of dose distribution of four-dimensional computed tomography (4DCT) simulation.
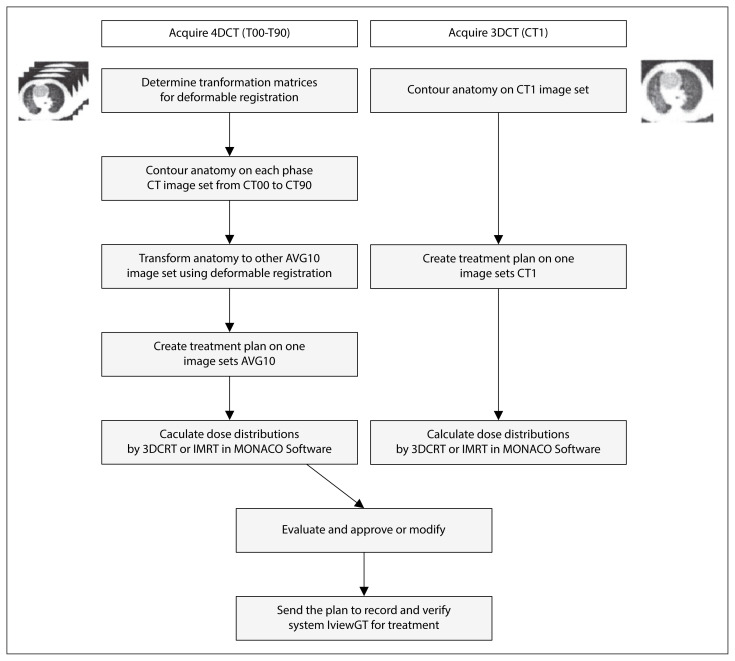
The gross tumor volume (GTV) and clinical target volume (CTV) were contoured in all 10 respiratory phases of 4DCT in 30 patients with non-small cell lung cancer (NSCLC). Both 3D and 4D treatment plans were made individually for each patient using the planning volume (PTV). The PTV3D was taken from a single CTV plus the recommended margin, and the PTV4D was taken from the 4D internal target volume, including all 10 CTVs plus the setup margins.
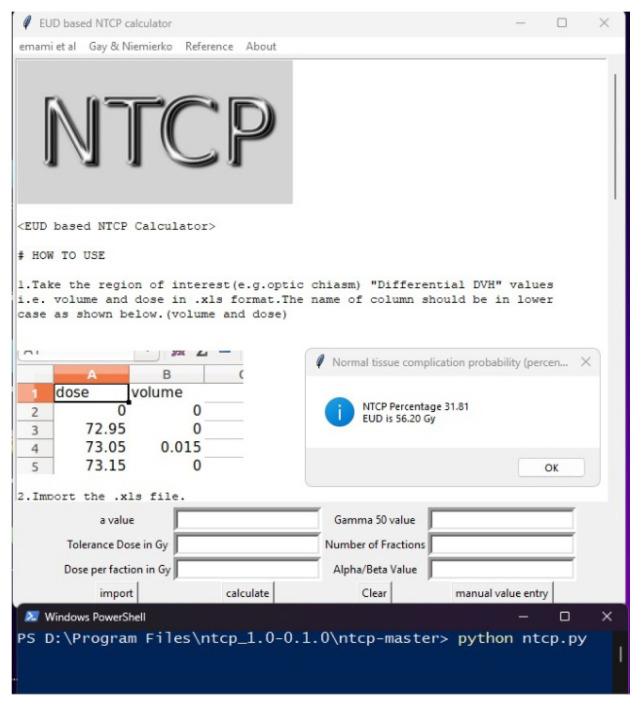
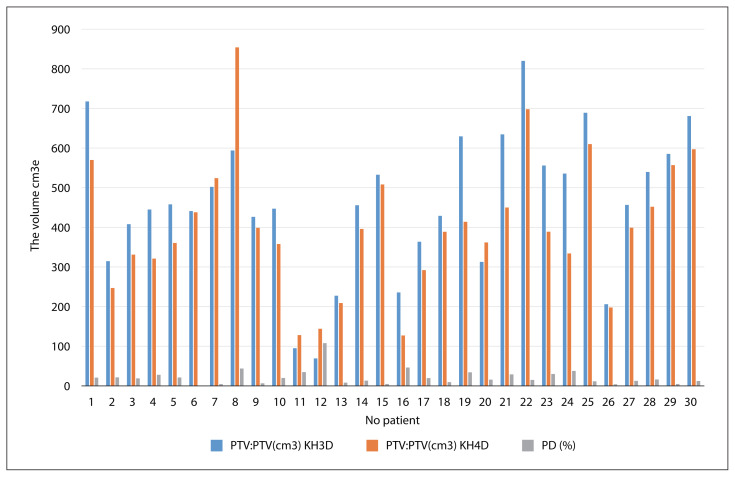
The mean PTV was 460 ± 179 (69-820) cm for 3DCT and 401 ± 167 (127-854) cm for 4DCT (p = 0.0018). The dose distribution (DD) of organs at risk, especially the lungs, was lower for the 4DCT simulation. The V5%, V10%, and V20% of the total lung dose for 4DCT were significantly lower for the 3DCT. However, lung V30% the heart, esophagus, and spinal cord were not significantly different. In addition, the conformity index and the dose heterogeneity index of the PTV were not significantly different. The normal tissue complication probability (NTCP) of the lung and heart was significantly lower for 4DCT than for 3DCT.
The 4DCT simulation gives better results on the NTCP. The organs at risk, especially the lungs, receive a significantly lower DD compared with the 3DCT. The conformity index (CI), heterogeneity index (HI) and the DD to the heart, spinal cord, and esophagus were not significantly different between the two techniques.
本研究旨在评估四维计算机断层扫描(4DCT)模拟剂量分布的有效性。
对30例非小细胞肺癌(NSCLC)患者的4DCT的所有10个呼吸期进行大体肿瘤体积(GTV)和临床靶体积(CTV)勾画。使用计划靶体积(PTV)分别为每位患者制定三维(3D)和四维(4D)治疗计划。PTV3D取自单个CTV加上推荐的边界,PTV4D取自4D内部靶体积,包括所有10个CTV加上摆位边界。
3DCT的平均PTV为460±179(69 - 820)cm³,4DCT的平均PTV为401±167(127 - 854)cm³(p = 0.0018)。4DCT模拟中危及器官的剂量分布(DD),尤其是肺部,更低。4DCT的全肺剂量的V5%、V10%和V20%显著低于3DCT。然而,肺V30%、心脏、食管和脊髓无显著差异。此外,PTV的适形指数和剂量不均匀性指数无显著差异。4DCT的肺和心脏的正常组织并发症概率(NTCP)显著低于3DCT。
4DCT模拟在NTCP方面给出了更好的结果。与3DCT相比,危及器官尤其是肺部接受的DD显著更低。两种技术之间的适形指数(CI)、不均匀性指数(HI)以及心脏、脊髓和食管的DD无显著差异。