The Medical Oncology Centre of Rosebank, 129 Oxford Road, Saxonwold 2196, Johannesburg, South Africa.
Department of Immunology, Faculty of Health Sciences, University of Pretoria, Pretoria, South Africa.
Support Care Cancer. 2023 Oct 13;31(12):628. doi: 10.1007/s00520-023-08071-0.
Limited knowledge is available on the incidence of febrile neutropenia (FN) in intermediate-risk patients and the rationale for use of granulocyte colony-stimulating factor (G-CSF) in these patients. We aimed to estimate the rate at which patients associated with intermediate risk (10-20%) of FN would develop ≥ 1 episode of FN with a commonly used chemotherapy regimen in clinical practice.
This prospective, real-world, observational, multinational, multicenter study (December 2016-October 2019) recruited patients with solid tumors or Hodgkin's/non-Hodgkin's lymphoma. Patients receiving chemotherapy with intermediate risk of FN, but not G-CSF as primary prophylaxis were included and observed for the duration of the chemotherapy (≤ 6 cycles and ≤ 30 days after the last chemotherapy administration).
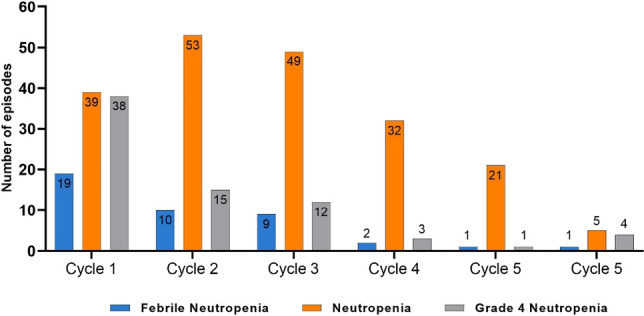
In total, 364 patients (median age, 56 years) with 1601 cycles of chemotherapy were included in the analysis. The incidence of FN was 5% in cycle 1, 3% in cycles 2-3, and 1% in cycles 4-6. The rate of patients with ≥ 1 episode of FN was 9%, and 59% of FN events were reported during cycle 1. The rate of grade 4 neutropenia in cycle 1 was 11%, and 15% of patients experienced ≥ 1 episode of grade 4 neutropenia.
Overall, the incidence of FN was low, with a high incidence in cycle 1 and a decrease in the subsequent cycles. These results provide the real FN risk for common chemotherapy regimens in patients generally excluded from clinical trials. Prophylactic G-CSF in intermediate-risk patients could be considered as per clinician's judgement.
关于中危(10-20%)患者中性粒细胞减少性发热(FN)的发生率以及在这些患者中使用粒细胞集落刺激因子(G-CSF)的原理知之甚少。我们旨在评估在临床实践中使用常用化疗方案时,与中危(10-20%)FN 相关的患者发生≥1 次 FN 发作的概率。
这是一项前瞻性、真实世界、观察性、多国家、多中心研究(2016 年 12 月至 2019 年 10 月),招募了患有实体瘤或霍奇金氏淋巴瘤/非霍奇金氏淋巴瘤的患者。纳入接受具有中危 FN 风险但不接受 G-CSF 作为一级预防的化疗的患者,并在化疗期间(≤6 个周期和≤最后一次化疗后 30 天)进行观察。
共有 364 名患者(中位年龄 56 岁)接受了 1601 个周期的化疗,纳入分析。第 1 周期 FN 的发生率为 5%,第 2-3 周期 FN 的发生率为 3%,第 4-6 周期 FN 的发生率为 1%。≥1 次 FN 发作的患者发生率为 9%,59%的 FN 事件发生在第 1 周期。第 1 周期的 4 级中性粒细胞减少发生率为 11%,15%的患者经历≥1 次 4 级中性粒细胞减少。
总体而言,FN 的发生率较低,第 1 周期发生率较高,随后周期发生率降低。这些结果为一般排除在临床试验之外的患者提供了常见化疗方案的真实 FN 风险。可根据临床医生的判断考虑在中危患者中预防性使用 G-CSF。