Derakhshan Arash, Männistö Tuija, Chen Liangmiao, Osinga Joris A J, Ashoor Ghalia, Lu Xuemian, Bliddal Sofie, Tao Fang-Biao, Brown Suzanne J, Vaidya Bijay, Hattersley Andrew T, Itoh Sachiko, Popova Polina V, Aminorroaya Ashraf, Kishi Reiko, Kianpour Maryam, Vasukova Elena A, López-Bermejo Abel, Oken Emily, Chatzi Leda, Vafeiadi Marina, Bramer Wichor M, Bassols Judit, Lertxundi Aitana, Fernández-Somoano Ana, Carrasco Paula, Auvinen Juha, Huang Kun, Feldt-Rasmussen Ulla, Grineva Elena N, Alexander Erik K, Pearce Elizabeth N, Chaker Layal, Walsh John P, Peeters Robin P, Guxens Mònica, Suvanto Eila, Nicolaides Kypros H, Korevaar Tim I M
Department of Internal Medicine, Erasmus University Medical Center, Rotterdam 3015 GD, The Netherlands.
Academic Center for Thyroid Diseases, Erasmus University Medical Center, Rotterdam 3015 GD, The Netherlands.
J Clin Endocrinol Metab. 2024 Feb 20;109(3):e1290-e1298. doi: 10.1210/clinem/dgad631.
Triiodothyronine (T3) is the bioactive form of thyroid hormone. In contrast to thyroid-stimulating hormone and free thyroxine, we lack knowledge on the association of gestational T3 with adverse obstetric outcomes.
To investigate the associaiton of gestational free or total T3 (FT3 or TT3) with adverse obstetric outcomes.
We collected individual participant data from prospective cohort studies on gestational FT3 or TT3, adverse obstetric outcomes (preeclampsia, gestational hypertension, preterm birth and very preterm birth, small for gestational age [SGA], and large for gestational age [LGA]), and potential confounders. We used mixed-effects regression models adjusting for potential confounders.
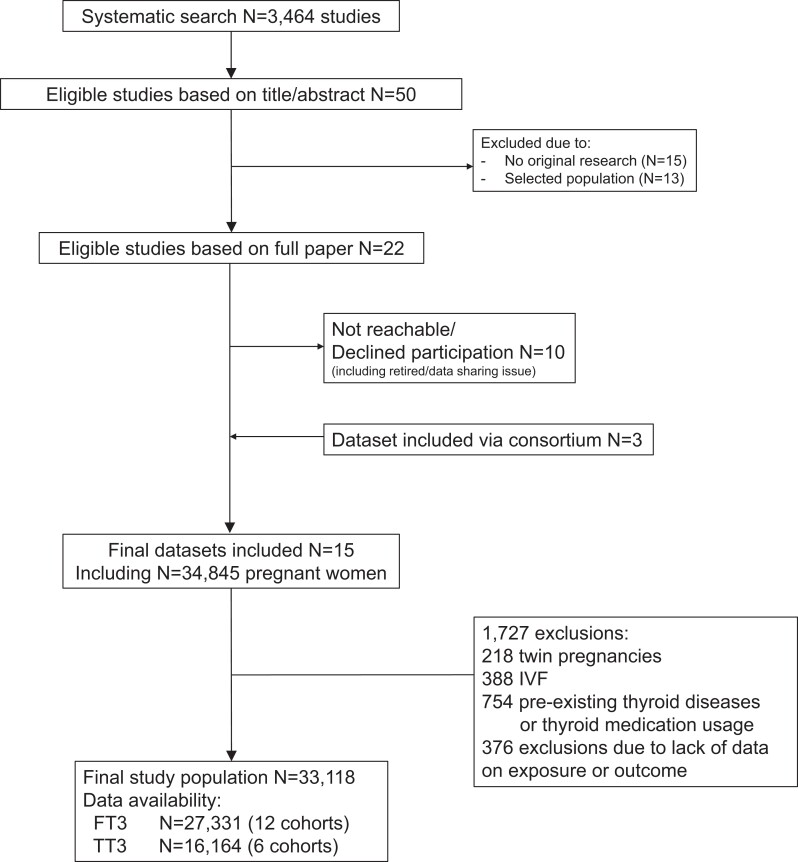
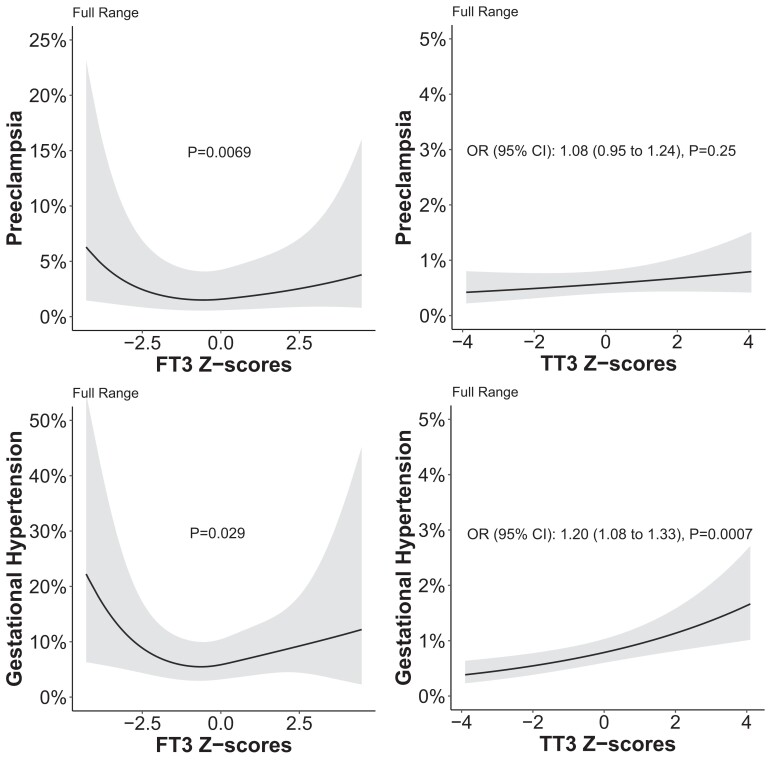
The final study population comprised 33 118 mother-child pairs of which 27 331 had data on FT3 and 16 164 on TT3. There was a U-shaped association of FT3 with preeclampsia (P = .0069) and a J-shaped association with the risk of gestational hypertension (P = .029). Higher TT3 was associated with a higher risk of gestational hypertension (OR per SD of TT3 1.20, 95% CI 1.08 to 1.33; P = .0007). A lower TT3 but not FT3 was associated with a higher risk of very preterm birth (OR 0.72, 95% CI 0.55 to 0.94; P = .018). TT3 but not FT3 was positively associated with birth weight (mean difference per 1 SD increase in TT3 12.8, 95% CI 6.5 to 19.1 g, P < .0001) but there was no association with SGA or LGA.
This study provides new insights on the association of gestational FT3 and TT3 with major adverse pregnancy outcomes that form the basis for future studies required to elucidate the effects of thyroid function on pregnancy outcomes. Based on the current study, routine FT3 or TT3 measurements for the assessment of thyroid function during pregnancy do not seem to be of added value in the risk assessment for adverse outcomes.
三碘甲状腺原氨酸(T3)是甲状腺激素的生物活性形式。与促甲状腺激素和游离甲状腺素不同,我们对孕期T3与不良产科结局之间的关联了解不足。
研究孕期游离或总T3(FT3或TT3)与不良产科结局之间的关联。
我们从关于孕期FT3或TT3、不良产科结局(先兆子痫、妊娠期高血压、早产和极早产、小于胎龄儿[SGA]和大于胎龄儿[LGA])以及潜在混杂因素的前瞻性队列研究中收集个体参与者数据。我们使用混合效应回归模型对潜在混杂因素进行调整。
最终研究人群包括33118对母婴,其中27331对有FT3数据,16164对有TT3数据。FT3与先兆子痫呈U型关联(P = 0.0069),与妊娠期高血压风险呈J型关联(P = 0.029)。较高的TT3与妊娠期高血压风险较高相关(TT3每标准差的比值比为1.20,95%置信区间为1.08至1.33;P = 0.0007)。较低的TT3而非FT3与极早产风险较高相关(比值比为0.72,95%置信区间为0.55至0.94;P = 0.018)。TT3而非FT3与出生体重呈正相关(TT3每增加1标准差的平均差异为12.8,95%置信区间为6.5至19.1克,P < 0.0001),但与SGA或LGA无关。
本研究为孕期FT3和TT3与主要不良妊娠结局之间的关联提供了新的见解,这些见解构成了未来阐明甲状腺功能对妊娠结局影响所需研究的基础。基于当前研究,孕期常规测量FT3或TT3以评估甲状腺功能在不良结局风险评估中似乎没有额外价值。