Kataoka Naoya, Imamura Teruhiko
Second Department of Internal Medicine, University of Toyama, 2630 Sugitani, Toyama 930-0194, Japan.
J Clin Med. 2023 Oct 18;12(20):6590. doi: 10.3390/jcm12206590.
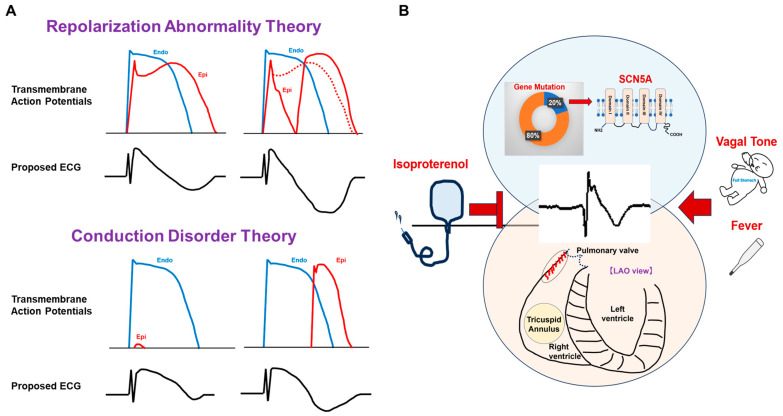
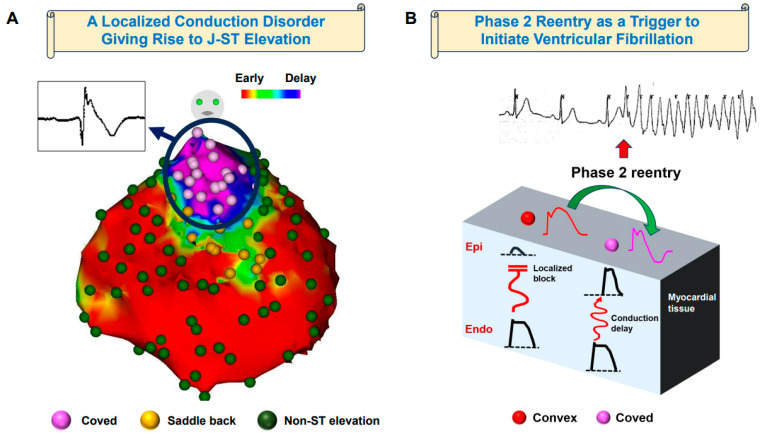
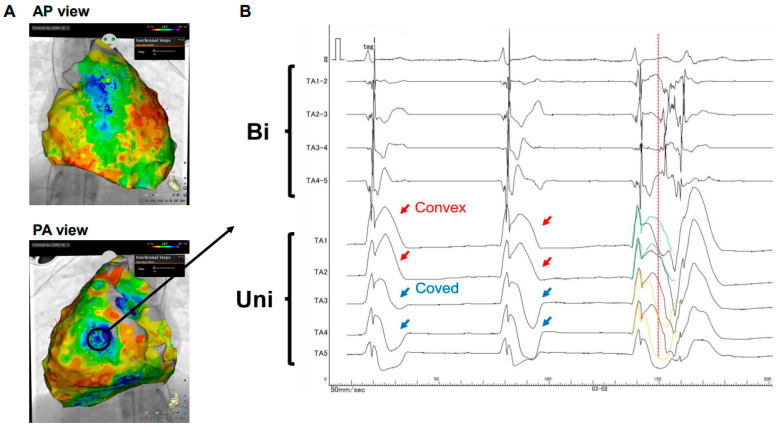
Brugada syndrome is characterized by pronounced J-ST segment elevation in the right precordial leads on surface electrocardiograms. The etiological underpinnings of these distinctive features have been the subject of extensive debate, encompassing various theories related to repolarization anomalies and conduction irregularities. Genetic investigations have unveiled SCN5A, the gene encoding NaV1.5, a critical sodium channel, as the most frequently implicated causative gene, with mutations typically manifesting as loss of function. Nonetheless, the detection rate of SCN5A mutations remains below 20%, underscoring the intricate genetic landscape of the syndrome. Histological analyses have divulged localized structural irregularities, primarily marked by fibrotic alterations, within the right ventricular outflow tract. Electrophysiological inquiries employing direct epicardial mapping techniques have uncovered localized conduction impediments concomitant with modifications in unipolar morphologies within the J-ST segment. Thus, the theory positing conduction abnormalities emerges as a compelling mechanism accounting for J-ST segment elevation. However, the precise mechanisms governing the onset of life-threatening tachyarrhythmias remain shrouded in uncertainty. Recent clinical case reports have proffered evidence supporting the notion that phase 2 reentry, arising from the marked heterogeneity in action potentials within the epicardial domain, may serve as the instigator of premature ventricular contractions, ultimately culminating in ventricular fibrillation. In light of these developments, it becomes increasingly evident that comprehending the mechanisms underlying the electrocardiographic manifestations and lethal arrhythmias in Brugada syndrome necessitates the consideration of a multifaceted perspective, transcending the binary discourse of repolarization versus depolarization anomalies.
Brugada综合征的特征是体表心电图上右胸前导联出现明显的J-ST段抬高。这些独特特征的病因基础一直是广泛争论的主题,涵盖了与复极异常和传导不规则相关的各种理论。基因研究揭示,编码关键钠通道NaV1.5的SCN5A基因是最常涉及的致病基因,其突变通常表现为功能丧失。然而,SCN5A突变的检出率仍低于20%,这突出了该综合征复杂的遗传格局。组织学分析揭示了右心室流出道内存在局部结构异常,主要表现为纤维化改变。采用直接心外膜标测技术的电生理研究发现,J-ST段存在局部传导障碍,同时单极形态也发生改变。因此,提出传导异常的理论成为解释J-ST段抬高的一个有说服力的机制。然而,危及生命的室性快速心律失常发作的确切机制仍不明朗。最近的临床病例报告提供了证据,支持这样一种观点,即心外膜区域动作电位的显著异质性引发的2期折返,可能是室性早搏的起因,最终导致心室颤动。鉴于这些进展,越来越明显的是,理解Brugada综合征心电图表现和致命性心律失常的潜在机制需要考虑多方面的观点,超越复极与去极异常的二元讨论。