Yu Dong-Mei, Wu Chun-Xiao, Sun Jun-Yi, Xue Hui, Yuwen Zhe, Feng Jiang-Xue
School of Nursing, Hebei University of Traditional Chinese Medicine, Shijiazhuang 050000, Hebei Province, China.
Department I of Anorectal, Hebei Traditional Chinese Medicine Hospital, Shijiazhuang 050000, Hebei Province, China.
World J Gastrointest Surg. 2023 Sep 27;15(9):1978-1985. doi: 10.4240/wjgs.v15.i9.1978.
Patients with colorectal cancer (CRC) are prone to stress ulcer after laparoscopic surgery. The analysis of risk factors for stress ulcer (SU) in patients with CRC is important to reduce mortality and improve patient prognosis.
To identify risk factors for SU after laparoscopic surgery for CRC, and develop a nomogram model to predict the risk of SU in these patients.
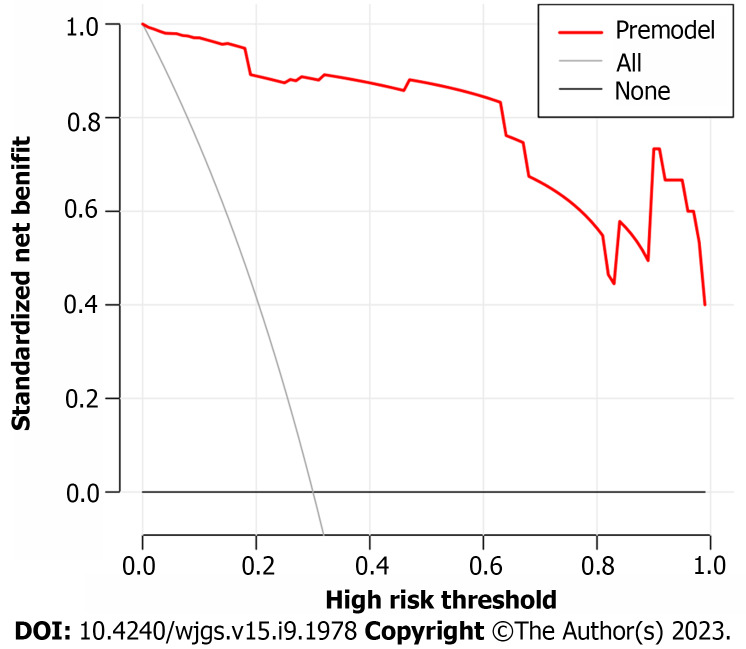
METHODSThe clinical data of 135 patients with CRC who underwent laparoscopic surgery between November 2021 and June 2022 were reviewed retrospectively. They were divided into two categories depending on the presence of SUs: The SU group ( = 23) and the non-SU group ( = 112). Univariate analysis and multivariate logistic regression analysis were used to screen for factors associated with postoperative SU in patients undergoing laparoscopic surgery, and a risk factor-based nomogram model was built based on these risk factors. By plotting the model's receiver operating characteristic (ROC) curve and calibration curve, a Hosmer-Lemeshow goodness of fit test was performed.
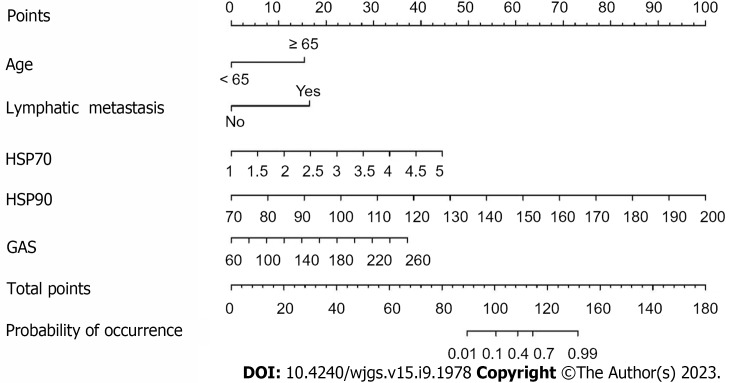
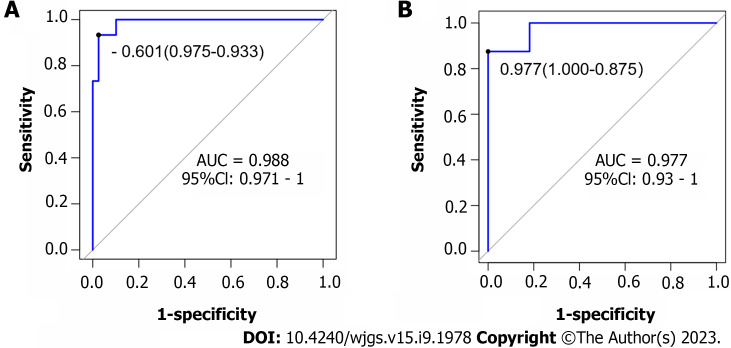
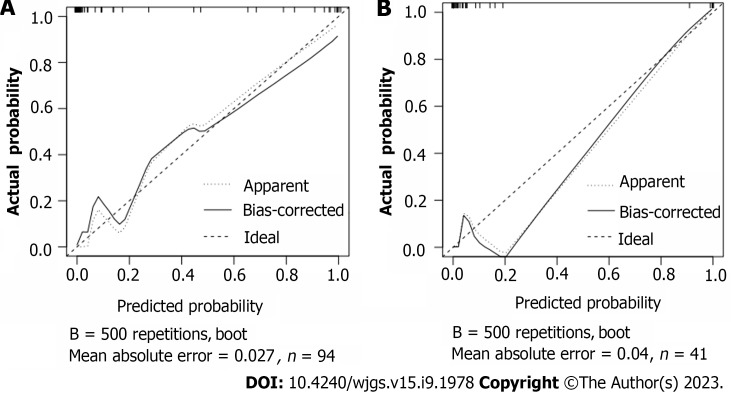
Among the 135 patients with CRC, 23 patients had postoperative SU, with an incidence of 17.04%. The SU group had higher levels of heat shock protein (HSP) 70, HSP90, and gastrin (GAS) than the non-SU group. Age, lymph node metastasis, HSP70, HSP90, and GAS levels were statistically different between the two groups, but other indicators were not statistically different. Logistic regression analysis showed that age ≥ 65 years, lymph node metastasis, and increased levels of HSP70, HSP90 and GAS were all risk factors for postoperative SU in patients with CRC ( < 0.05). According to these five risk factors, the area under the ROC curve for the nomogram model was 0.988 (95%CI: 0.971-1.0); the calibration curve demonstrated excellent agreement between predicted and actual probabilities, and the Hosmer-Lemeshow goodness of fit test revealed that the difference was not statistically significant ( = 0.753, = 0.999), suggesting that the nomogram model had good discrimination, calibration, and stability.
Patients with CRC aged ≥ 65 years, with lymph node metastasis and elevated HSP70, HSP90, GAS levels, are prone to post-laparoscopic surgery SU. Our nomogram model shows good predictive value.
结直肠癌(CRC)患者在腹腔镜手术后易发生应激性溃疡。分析CRC患者应激性溃疡(SU)的危险因素对于降低死亡率和改善患者预后具有重要意义。
确定CRC腹腔镜手术后SU的危险因素,并建立列线图模型以预测这些患者发生SU的风险。
回顾性分析2021年11月至2022年6月期间接受腹腔镜手术的135例CRC患者的临床资料。根据是否存在SU将他们分为两类:SU组(n = 23)和非SU组(n = 112)。采用单因素分析和多因素逻辑回归分析筛选腹腔镜手术患者术后SU的相关因素,并基于这些危险因素建立基于风险因素的列线图模型。通过绘制模型的受试者工作特征(ROC)曲线和校准曲线,进行Hosmer-Lemeshow拟合优度检验。
135例CRC患者中,23例术后发生SU,发生率为17.04%。SU组的热休克蛋白(HSP)70、HSP90和胃泌素(GAS)水平高于非SU组。两组患者的年龄、淋巴结转移、HSP70、HSP90和GAS水平差异有统计学意义,但其他指标差异无统计学意义。逻辑回归分析显示,年龄≥65岁、淋巴结转移以及HSP70、HSP90和GAS水平升高均是CRC患者术后SU的危险因素(P < 0.05)。根据这五个危险因素,列线图模型的ROC曲线下面积为0.988(95%CI:0.971 - 1.0);校准曲线显示预测概率与实际概率之间具有良好的一致性,Hosmer-Lemeshow拟合优度检验显示差异无统计学意义(χ² = 0.753,P = 0.999),表明列线图模型具有良好的区分度、校准度和稳定性。
年龄≥65岁、有淋巴结转移且HSP70、HSP90、GAS水平升高的CRC患者在腹腔镜手术后易发生SU。我们的列线图模型具有良好的预测价值。