Department of Intensive Care Medicine, HwaMei Hospital, University Of Chinese Academy of Sciences, Ningbo, 315000, Zhejiang, China.
Department of Emergency, Ningbo Yinzhou No.2 Hospital, Ningbo, 315000, Zhejiang, China.
BMC Gastroenterol. 2019 Nov 21;19(1):193. doi: 10.1186/s12876-019-1105-y.
Proton pump inhibitors (PPI) and histamine 2 receptor antagonists (H2RA) have been widely used as stress ulcer prophylaxis (SUP) in critically ill patients, however, its efficacy and safety remain unclear. This study aimed to assess the effect of SUP on clinical outcomes in critically ill adults.
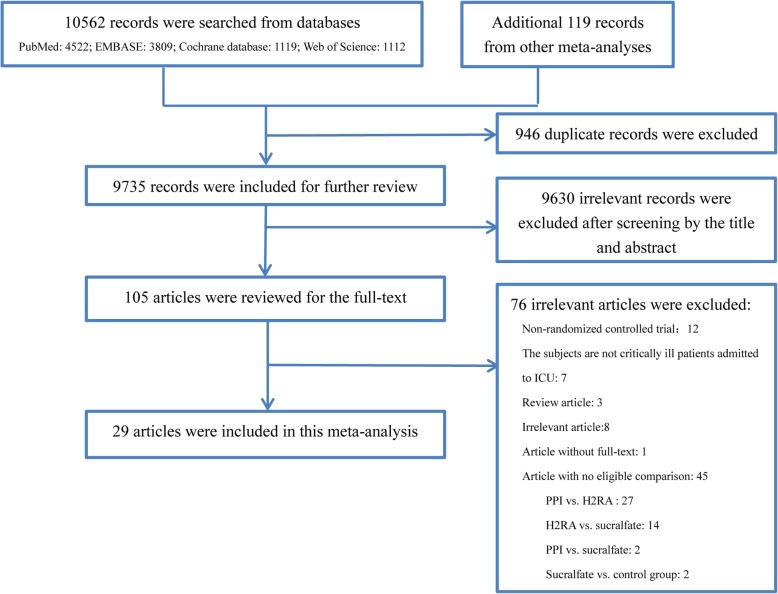
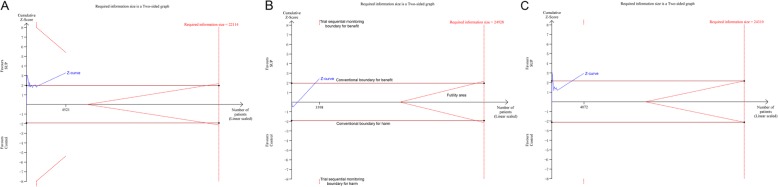
Literature search was conducted in PubMed, EMBASE, Web of Science, and the Cochrane database of clinical trials for randomized controlled trials (RCTs) that investigated SUP, with PPI or H2RA, versus placebo or no prophylaxis in critically ill patients from database inception through 1 June 2019. Study selection, data extraction and quality assessment were performed in duplicate. The primary outcomes were clinically important gastrointestinal (GI) bleeding and overt GI bleeding. Conventional meta-analysis with random-effects model and trial sequential analysis (TSA) were performed.
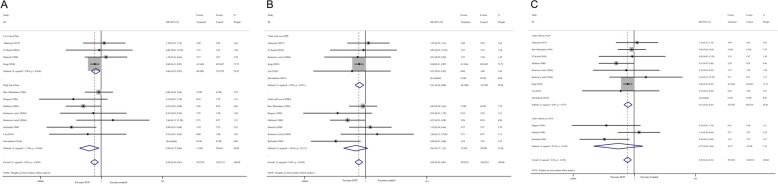
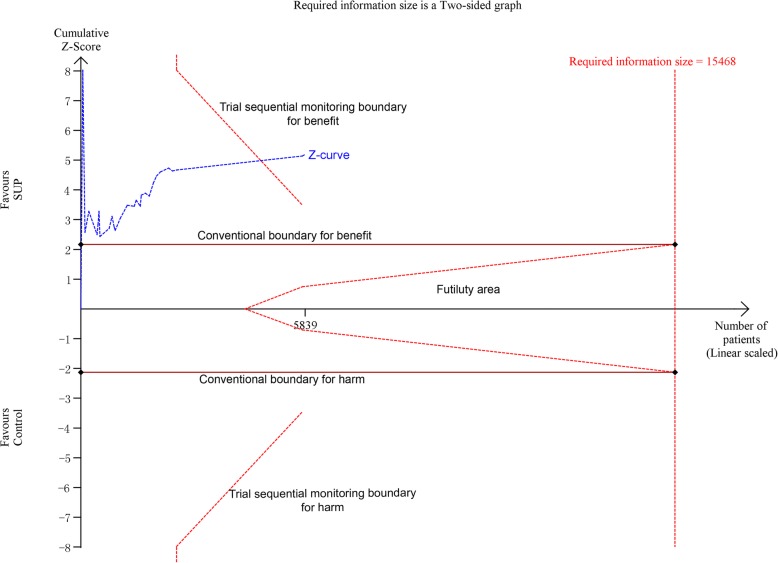
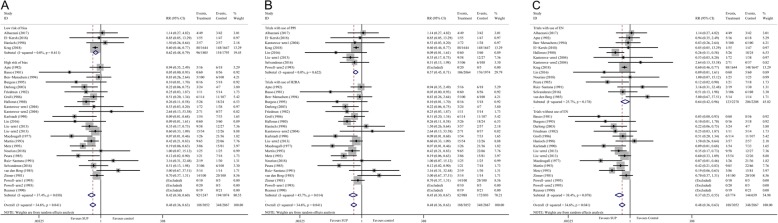
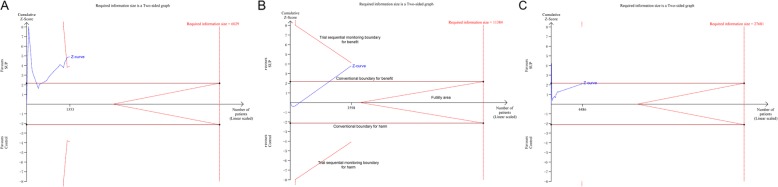
Twenty-nine RCTs were identified, of which four RCTs were judged as low risk of bias. Overall, SUP could reduce the incident of clinically important GI bleeding [relative risk (RR) = 0.58; 95% confidence intervals (CI): 0.42-0.81] and overt GI bleeding (RR = 0.48; 95% CI: 0.36-0.63), these results were confirmed by the sub-analysis of trials with low risk of bias, TSA indicated a firm evidence on its beneficial effects on the overt GI bleeding (TSA-adjusted CI: 0.31-0.75), but lack of sufficient evidence on the clinically important GI bleeding (TSA-adjusted CI: 0.23-1.51). Among patients who received enteral nutrition (EN), SUP was associated with a decreased risk of clinically important GI bleeding (RR = 0.61; 95% CI: 0.44-0.85; TSA-adjusted CI: 0.16-2.38) and overt GI bleeding (RR = 0.64; 95% CI: 0.42-0.96; TSA-adjusted CI: 0.12-3.35), but these benefits disappeared after adjustment with TSA. Among patients who did not receive EN, SUP had only benefits in reducing the risk of overt GI bleeding (RR = 0.37; 95% CI: 0.25-0.55; TSA-adjusted CI: 0.22-0.63), but not the clinically important GI bleeding (RR = 0.27; 95% CI: 0.04-2.09).
SUP has benefits on the overt GI bleeding in critically ill patients who did not receive EN, however, its benefits on clinically important GI bleeding still needs more evidence to confirm.
质子泵抑制剂(PPI)和组胺 2 受体拮抗剂(H2RA)已被广泛用于重症患者的应激性溃疡预防(SUP),但其疗效和安全性仍不清楚。本研究旨在评估 SUP 对重症成人临床结局的影响。
对 PubMed、EMBASE、Web of Science 和 Cochrane 临床试验数据库进行文献检索,以纳入研究 SUP(使用 PPI 或 H2RA)与安慰剂或无预防措施相比,在重症患者中的随机对照试验(RCT)。研究选择、数据提取和质量评估均由两人进行。主要结局为临床相关胃肠道(GI)出血和显性 GI 出血。采用随机效应模型进行常规荟萃分析和试验序贯分析(TSA)。
共确定了 29 项 RCT,其中 4 项 RCT 被评为低偏倚风险。总体而言,SUP 可降低临床相关 GI 出血的发生率[相对风险(RR)=0.58;95%置信区间(CI):0.42-0.81]和显性 GI 出血(RR=0.48;95%CI:0.36-0.63),这些结果在低偏倚风险试验的亚组分析中得到证实,TSA 表明其对显性 GI 出血有确凿的有益作用(TSA 调整 CI:0.31-0.75),但对临床相关 GI 出血的证据不足(TSA 调整 CI:0.23-1.51)。在接受肠内营养(EN)的患者中,SUP 与临床相关 GI 出血风险降低相关(RR=0.61;95%CI:0.44-0.85;TSA 调整 CI:0.16-2.38)和显性 GI 出血(RR=0.64;95%CI:0.42-0.96;TSA 调整 CI:0.12-3.35),但这些益处在用 TSA 调整后消失。在未接受 EN 的患者中,SUP 仅能降低显性 GI 出血的风险(RR=0.37;95%CI:0.25-0.55;TSA 调整 CI:0.22-0.63),但对临床相关 GI 出血没有益处(RR=0.27;95%CI:0.04-2.09)。
SUP 对未接受 EN 的重症患者显性 GI 出血有获益,但对临床相关 GI 出血的获益仍需要更多证据证实。