Department of Radiology, Faculty of Medicine and University Hospital Cologne, University of Cologne, Cologne, Germany.
Department of Cardiology, Heart Center, Faculty of Medicine, University of Cologne, Cologne, Germany.
Eur Radiol. 2024 May;34(5):2944-2956. doi: 10.1007/s00330-023-10337-4. Epub 2023 Nov 3.
To evaluate dual-layer dual-energy computed tomography (dlDECT)-derived pulmonary perfusion maps for differentiation between acute pulmonary embolism (PE) and chronic thromboembolic pulmonary hypertension (CTEPH).
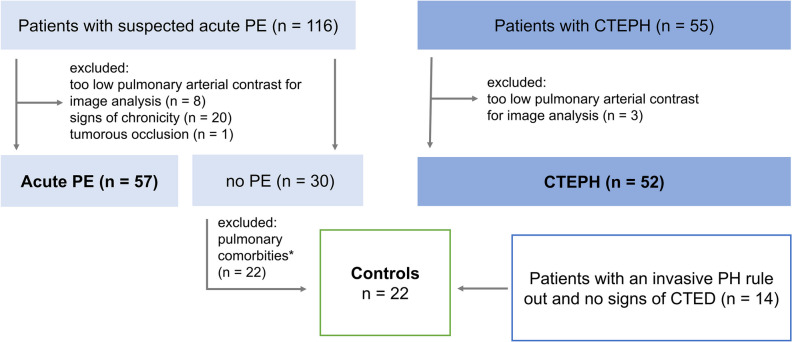
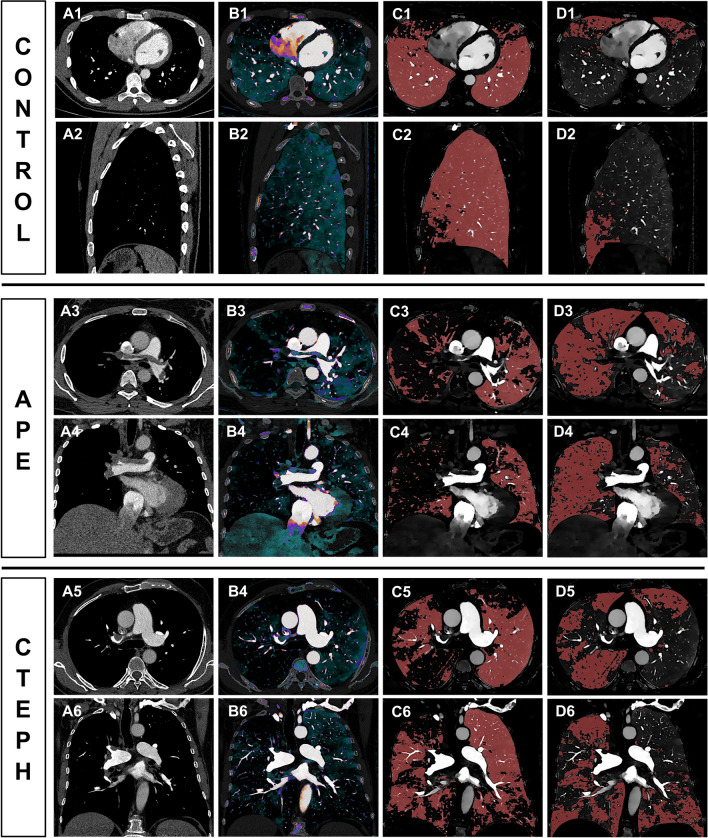
This retrospective study included 131 patients (57 patients with acute PE, 52 CTEPH, 22 controls), who underwent CT pulmonary angiography on a dlDECT. Normal and malperfused areas of lung parenchyma were semiautomatically contoured using iodine density overlay (IDO) maps. First-order histogram features of normal and malperfused lung tissue were extracted. Iodine density (ID) was normalized to the mean pulmonary artery (MPA) and the left atrium (LA). Furthermore, morphological imaging features for both acute and chronic PE, as well as the combination of histogram and morphological imaging features, were evaluated.
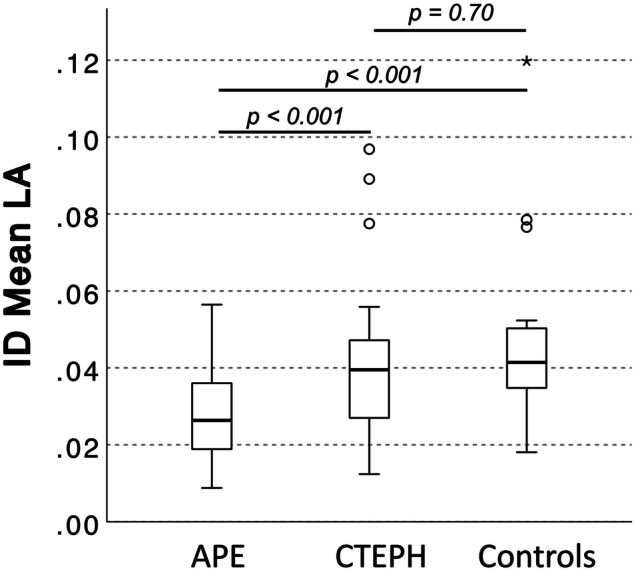
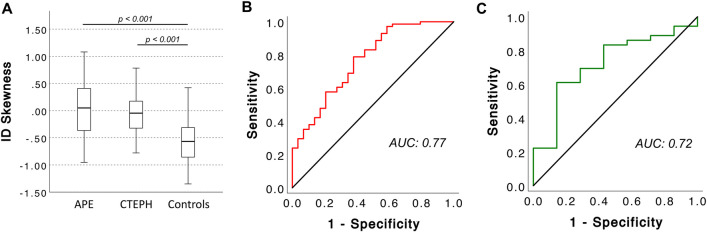
In acute PE, normal perfused lung areas showed a higher mean and peak iodine uptake normalized to the MPA than in CTEPH (both p < 0.001). After normalizing mean ID in perfusion defects to the LA, patients with acute PE had a reduced average perfusion (ID) compared to both CTEPH patients and controls (p < 0.001 for both). ID allowed for a differentiation between acute PE and CTEPH with moderate accuracy (AUC: 0.72, sensitivity 74%, specificity 64%), resulting in a PPV and NPV for CTEPH of 64% and 70%. Combining ID in the malperfused areas with the diameter of the MPA (MPA) significantly increased its ability to differentiate between acute PE and CTEPH (sole MPA: AUC: 0.76, 95%-CI: 0.68-0.85 vs. MPA + 256.3 * ID - 40.0: AUC: 0.82, 95%-CI: 0.74-0.90, p = 0.04).
dlDECT enables quantification and characterization of pulmonary perfusion patterns in acute PE and CTEPH. Although these lack precision when used as a standalone criterion, when combined with morphological CT parameters, they hold potential to enhance differentiation between the two diseases.
Differentiating between acute PE and CTEPH based on morphological CT parameters is challenging, often leading to a delay in CTEPH diagnosis. By revealing distinct pulmonary perfusion patterns in both entities, dlDECT may facilitate timely diagnosis of CTEPH, ultimately improving clinical management.
• Morphological imaging parameters derived from CT pulmonary angiography to distinguish between acute pulmonary embolism and chronic thromboembolic pulmonary hypertension lack diagnostic accuracy. • Dual-layer dual-energy CT reveals different pulmonary perfusion patterns between acute pulmonary embolism and chronic thromboembolic pulmonary hypertension. • The identified parameters yield potential to enable more timely identification of patients with chronic thromboembolic pulmonary hypertension.
评估双层双能 CT(dlDECT)衍生的肺灌注图,以区分急性肺栓塞(PE)和慢性血栓栓塞性肺动脉高压(CTEPH)。
这项回顾性研究纳入了 131 名患者(57 名急性 PE 患者、52 名 CTEPH 患者、22 名对照组),他们在 dlDECT 上进行了 CT 肺动脉造影。使用碘密度叠加(IDO)图半自动勾绘肺实质的正常和灌注不良区域。提取正常和灌注不良肺组织的一阶直方图特征。碘密度(ID)归一化为肺动脉(MPA)和左心房(LA)。此外,评估了急性和慢性 PE 的形态学成像特征,以及直方图和形态学成像特征的组合。
在急性 PE 中,正常灌注的肺区的平均和峰值碘摄取值与 CTEPH 相比均更高(均 P < 0.001)。在将灌注缺陷中的平均 ID 归一化为 LA 后,急性 PE 患者的平均灌注(ID)与 CTEPH 患者和对照组相比均降低(均 P < 0.001)。ID 可实现急性 PE 和 CTEPH 的中等准确性区分(AUC:0.72,灵敏度 74%,特异性 64%),导致 CTEPH 的阳性预测值和阴性预测值分别为 64%和 70%。将灌注不良区域中的 ID 与 MPA(MPA)的直径结合使用可显著提高其区分急性 PE 和 CTEPH 的能力(单独 MPA:AUC:0.76,95%-CI:0.68-0.85 与 MPA + 256.3 * ID - 40.0:AUC:0.82,95%-CI:0.74-0.90,P = 0.04)。
dlDECT 可实现急性 PE 和 CTEPH 肺灌注模式的定量和特征描述。虽然单独使用时精度不足,但与形态学 CT 参数结合使用时,它们具有增强两种疾病之间区分的潜力。
基于形态学 CT 参数区分急性 PE 和 CTEPH 具有挑战性,通常会导致 CTEPH 诊断延迟。通过揭示两种实体之间不同的肺灌注模式,dlDECT 可能有助于更及时地诊断 CTEPH,从而最终改善临床管理。
• 从 CT 肺动脉造影中得出的区分急性肺栓塞和慢性血栓栓塞性肺动脉高压的形态学成像参数缺乏诊断准确性。• 双层双能 CT 揭示了急性肺栓塞和慢性血栓栓塞性肺动脉高压之间不同的肺灌注模式。• 所识别的参数具有使患者更及时地识别慢性血栓栓塞性肺动脉高压的潜力。