Shamas Mohamad, Yeh Hsiang J, Fried Itzhak, Engel Jerome, Staba Richard J
David Geffen School of Medicine at UCLA, Los Angeles, CA 90095, USA.
Brain Commun. 2023 Oct 24;5(6):fcad289. doi: 10.1093/braincomms/fcad289. eCollection 2023.
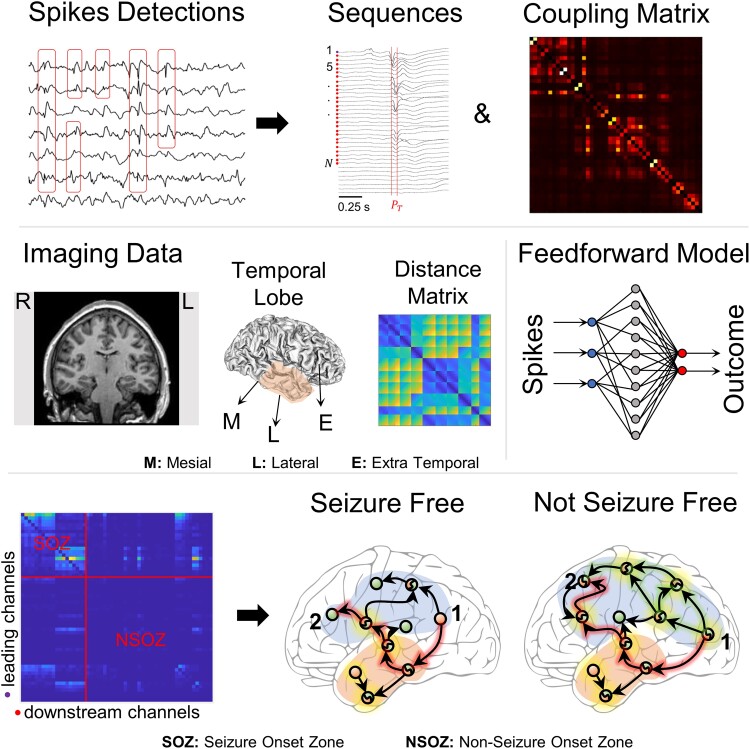
Inter-ictal spikes aid in the diagnosis of epilepsy and in planning surgery of medication-resistant epilepsy. However, the localizing information from spikes can be unreliable because spikes can propagate, and the burden of spikes, often assessed as a rate, does not always correlate with the seizure onset zone or seizure outcome. Recent work indicates identifying where spikes regularly emerge and spread could localize the seizure network. Thus, the current study sought to better understand where and how rates of single and coupled spikes, and especially brain regions with high-rate and leading spike of a propagating sequence, informs the extent of the seizure network. In 37 patients with medication-resistant temporal lobe seizures, who had surgery to treat their seizure disorder, an algorithm detected spikes in the pre-surgical depth inter-ictal EEG. A separate algorithm detected spike propagation sequences and identified the location of leading and downstream spikes in each sequence. We analysed the rate and power of single spikes on each electrode and coupled spikes between pairs of electrodes, and the proportion of sites with high-rate, leading spikes in relation to the seizure onset zone of patients seizure free ( = 19) and those with continuing seizures ( = 18). We found increased rates of single spikes in mesial temporal seizure onset zone (ANOVA, < 0.001, = 0.138), and increased rates of coupled spikes within, but not between, mesial-, lateral- and extra-temporal seizure onset zone of patients with continuing seizures ( < 0.001; = 0.195, 0.113 and 0.102, respectively). In these same patients, there was a higher proportion of brain regions with high-rate leaders, and each sequence contained a greater number of spikes that propagated with a higher efficiency over a longer distance outside the seizure onset zone than patients seizure free (Wilcoxon, = 0.0172). The proportion of high-rate leaders in and outside the seizure onset zone could predict seizure outcome with area under curve = 0.699, but not rates of single or coupled spikes (0.514 and 0.566). Rates of coupled spikes to a greater extent than single spikes localize the seizure onset zone and provide evidence for inter-ictal functional segregation, which could be an adaptation to avert seizures. Spike rates, however, have little value in predicting seizure outcome. High-rate spike sites leading propagation could represent sources of spikes that are important components of an efficient seizure network beyond the clinical seizure onset zone, and like the seizure onset zone these, too, need to be removed, disconnected or stimulated to increase the likelihood for seizure control.
发作间期棘波有助于癫痫的诊断以及药物难治性癫痫手术的规划。然而,棘波提供的定位信息可能不可靠,因为棘波能够传播,而且通常以频率评估的棘波负担并不总是与癫痫发作起始区或癫痫发作结果相关。最近的研究表明,确定棘波经常出现和传播的位置可以定位癫痫发作网络。因此,本研究旨在更好地了解单个和耦合棘波的频率在何处以及如何发挥作用,特别是具有高频和传播序列领先棘波的脑区,如何反映癫痫发作网络的范围。在37例接受手术治疗癫痫发作障碍的药物难治性颞叶癫痫患者中,一种算法检测术前深部发作间期脑电图中的棘波。另一种算法检测棘波传播序列,并确定每个序列中领先和下游棘波的位置。我们分析了每个电极上单个棘波的频率和功率以及电极对之间的耦合棘波,以及在癫痫发作已缓解(n = 19)和仍有癫痫发作(n = 18)的患者中,具有高频领先棘波的部位相对于癫痫发作起始区的比例。我们发现内侧颞叶癫痫发作起始区单个棘波频率增加(方差分析,P < 0.001,η² = 0.138),仍有癫痫发作的患者在内侧、外侧和颞外癫痫发作起始区内但不是区与区之间耦合棘波频率增加(P < 0.001;η²分别为0.195、0.113和0.102)。在这些相同的患者中,具有高频领先棘波的脑区比例更高,并且与癫痫发作已缓解的患者相比,每个序列包含更多数量的棘波,这些棘波在癫痫发作起始区外以更高的效率传播更长的距离(Wilcoxon检验,P = 0.017)。癫痫发作起始区内和外高频领先棘波的比例可以预测癫痫发作结果,曲线下面积为0.699,但单个或耦合棘波的频率则不能(分别为0.514和0.566)。耦合棘波频率比单个棘波频率在更大程度上定位癫痫发作起始区,并为发作间期功能分离提供证据,这可能是一种预防癫痫发作的适应性机制。然而,棘波频率在预测癫痫发作结果方面价值不大。领先传播的高频棘波部位可能代表棘波源,这些棘波源是临床癫痫发作起始区之外有效癫痫发作网络的重要组成部分,与癫痫发作起始区一样,这些部位也需要被切除、离断或刺激,以增加癫痫控制的可能性。