La Rosa Riccardo, Grechi Benedetta, Ragazzi Riccardo, Alvisi Valentina, Montanari Giacomo, Marangoni Elisabetta, Volta Carlo Alberto, Spadaro Savino, Scaramuzzo Gaetano
Department of Translational Medicine and for Romagna, University of Ferrara, 44124 Ferrara, Italy.
Anesthesia and Intensive Care Unit, Emergency Department, Azienda Ospedaliera Universitaria Ferrara, 44124 Ferrara, Italy.
Healthcare (Basel). 2023 Nov 4;11(21):2903. doi: 10.3390/healthcare11212903.
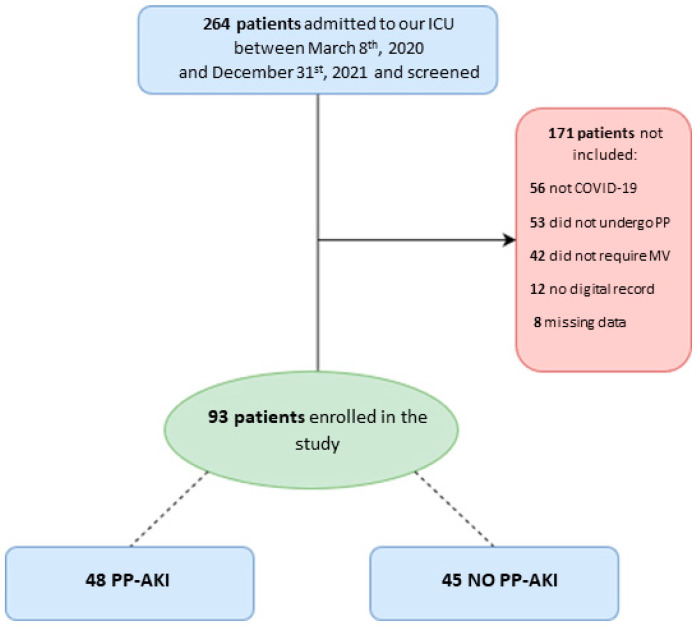
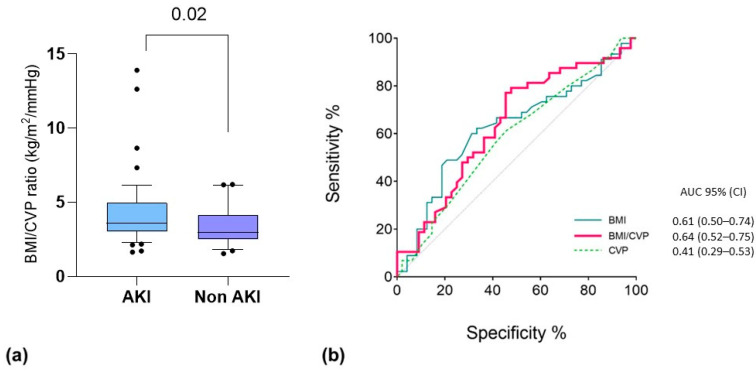
(1) Background: Acute kidney injury (AKI) is common among critically ill COVID-19 patients, but its temporal association with prone positioning (PP) is still unknown, and no data exist on the possibility of predicting PP-associated AKI from bedside clinical variables. (2) Methods: We analyzed data from 93 COVID-19-related ARDS patients who underwent invasive mechanical ventilation (IMV) and at least one PP cycle. We collected hemodynamic variables, respiratory mechanics, and circulating biomarkers before, during, and after the first PP cycle. PP-associated AKI (PP-AKI) was defined as AKI diagnosed any time from the start of PP to 48 h after returning to the supine position. A -test for independent samples was used to test for the differences between groups, while binomial logistical regression was performed to assess variables independently associated with PP-associated AKI. (3) Results: A total of 48/93 (52%) patients developed PP-AKI, with a median onset at 24 [13.5-44.5] hours after starting PP. No significant differences in demographic characteristics between groups were found. Before starting the first PP cycle, patients who developed PP-AKI had a significantly lower cumulative fluid balance (CFB), even when normalized for body weight ( = 0.006). Central venous pressure (CVP) values, measured before the first PP (OR 0.803, 95% CI [0.684-0.942], = 0.007), as well as BMI (OR 1.153, 95% CI = [1.013-1.313], = 0.031), were independently associated with the development of PP-AKI. In the multivariable regression analysis, a lower CVP before the first PP cycle was independently associated with ventilator-free days (OR 0.271, 95% CI [0.123-0.936], = 0.011) and with ICU mortality (OR:0.831, 95% CI [0.699-0.989], = 0.037). (4) Conclusions: Acute kidney injury occurs frequently in invasively ventilated severe COVID-19 ARDS patients undergoing their first prone positioning cycle. Higher BMI and lower CVP before PP are independently associated with the occurrence of AKI during prone positioning.
(1) 背景:急性肾损伤(AKI)在危重症COVID-19患者中很常见,但其与俯卧位通气(PP)的时间关联仍不清楚,且尚无关于能否根据床边临床变量预测PP相关AKI的数据。(2) 方法:我们分析了93例接受有创机械通气(IMV)且经历至少一个PP周期的COVID-19相关急性呼吸窘迫综合征(ARDS)患者的数据。我们在第一个PP周期之前、期间和之后收集了血流动力学变量、呼吸力学和循环生物标志物。PP相关AKI(PP-AKI)定义为从PP开始至恢复仰卧位后48小时内任何时间诊断出的AKI。采用独立样本t检验来检验组间差异,同时进行二项逻辑回归以评估与PP相关AKI独立相关的变量。(3) 结果:共有48/93(52%)例患者发生PP-AKI,中位发病时间为开始PP后24[13.5 - 44.5]小时。两组间人口统计学特征无显著差异。在开始第一个PP周期之前,发生PP-AKI的患者累积液体平衡(CFB)显著更低,即使按体重进行标准化后也是如此(P = 0.006)。第一个PP之前测量的中心静脉压(CVP)值(OR 0.803,95%CI[0.684 - 0.942],P = 0.007)以及体重指数(BMI)(OR 1.153,95%CI = [1.013 - 1.313],P = 0.031)与PP-AKI的发生独立相关。在多变量回归分析中,第一个PP周期之前较低的CVP与无呼吸机天数独立相关(OR 0.271,95%CI[0.123 - 0.936],P = 0.011)以及与ICU死亡率相关(OR:0.831,95%CI[0.699 - 0.989],P = 0.037)。(4) 结论:在接受首次俯卧位通气周期的有创通气的重症COVID-19 ARDS患者中,急性肾损伤频繁发生。PP之前较高的BMI和较低的CVP与俯卧位期间AKI的发生独立相关。