Verville Leslie, Ogilvie Rachel, Hincapié Cesar A, Southerst Danielle, Yu Hainan, Bussières André, Gross Douglas P, Pereira Paulo, Mior Silvano, Tricco Andrea C, Cedraschi Christine, Brunton Ginny, Nordin Margareta, Connell Gaelan, Wong Jessica J, Shearer Heather M, Lee Joyce G B, Wang Dan, Hayden Jill A, Cancelliere Carol
Institute for Disability and Rehabilitation Research and Faculty of Health Sciences, Ontario Tech University, Oshawa, Canada.
Department of Community Health and Epidemiology, Dalhousie University, Halifax, Canada.
J Occup Rehabil. 2023 Dec;33(4):636-650. doi: 10.1007/s10926-023-10124-4. Epub 2023 Nov 22.
Evaluate benefits and harms of structured exercise programs for chronic primary low back pain (CPLBP) in adults to inform a World Health Organization (WHO) standard clinical guideline.
We searched for randomized controlled trials (RCTs) in electronic databases (inception to 17 May 2022). Eligible RCTs targeted structured exercise programs compared to placebo/sham, usual care, or no intervention (including comparison interventions where the attributable effect of exercise could be isolated). We extracted outcomes, appraised risk of bias, conducted meta-analyses where appropriate, and assessed certainty of evidence using GRADE.
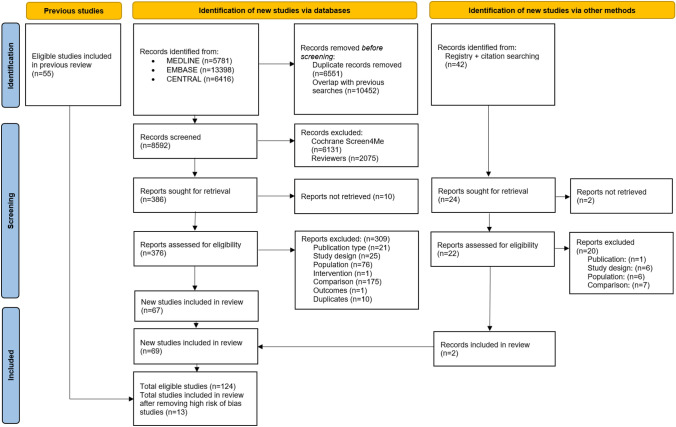
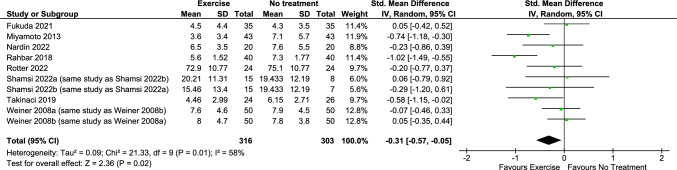
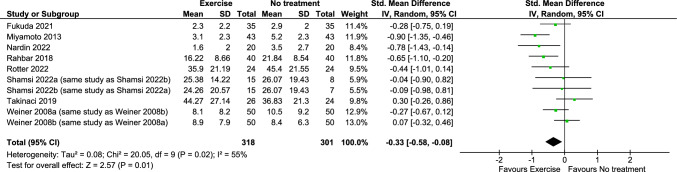
We screened 2503 records (after initial screening through Cochrane RCT Classifier and Cochrane Crowd) and 398 full text RCTs. Thirteen RCTs rated with overall low or unclear risk of bias were synthesized. Assessing individual exercise types (predominantly very low certainty evidence), pain reduction was associated with aerobic exercise and Pilates vs. no intervention, and motor control exercise vs. sham. Improved function was associated with mixed exercise vs. usual care, and Pilates vs. no intervention. Temporary increased minor pain was associated with mixed exercise vs. no intervention, and yoga vs. usual care. Little to no difference was found for other comparisons and outcomes. When pooling exercise types, exercise vs. no intervention probably reduces pain in adults (8 RCTs, SMD = - 0.33, 95% CI - 0.58 to - 0.08) and functional limitations in adults and older adults (8 RCTs, SMD = - 0.31, 95% CI - 0.57 to - 0.05) (moderate certainty evidence).
With moderate certainty, structured exercise programs probably reduce pain and functional limitations in adults and older people with CPLBP.
评估成人慢性原发性下腰痛(CPLBP)结构化运动计划的益处和危害,为世界卫生组织(WHO)标准临床指南提供依据。
我们在电子数据库中检索随机对照试验(RCT)(从数据库建立至2022年5月17日)。符合条件的RCT针对结构化运动计划,与安慰剂/假干预、常规护理或无干预进行比较(包括可分离运动归因效应的比较干预)。我们提取了结果,评估了偏倚风险,在适当情况下进行了荟萃分析,并使用GRADE评估了证据的确定性。
我们筛选了2503条记录(通过Cochrane RCT分类器和Cochrane Crowd进行初步筛选后)和398篇全文RCT。综合了13项偏倚风险总体较低或不明确的RCT。评估个体运动类型(主要是极低确定性证据)时,与无干预相比,有氧运动和普拉提与疼痛减轻相关,运动控制训练与假干预相比与疼痛减轻相关。与常规护理相比,混合运动与功能改善相关,与无干预相比,普拉提与功能改善相关。与无干预相比,混合运动和与常规护理相比瑜伽与轻微疼痛暂时增加相关。其他比较和结果几乎没有差异。汇总运动类型时,运动与无干预相比可能会减轻成人疼痛(8项RCT,标准化均数差(SMD)=-0.33,95%置信区间(CI)-0.58至-0.08)以及成人和老年人的功能受限(8项RCT,SMD=-0.31,95%CI-0.57至-0.05)(中等确定性证据)。
中等确定性下,结构化运动计划可能会减轻CPLBP成人和老年人的疼痛及功能受限。