Laboratory of Clinical and Epidemiological Virology (Rega Institute), Department of Microbiology, Immunology and Transplantation, Rega Institute for Medical Research Clinical and Epidemiological Virology, Institute for the Future, KU Leuven, Rega-Herestraat 49-Bus 1040, 3000, Leuven, Belgium.
Department of Pharmaceutical Microbiology, School of Pharmacy, Muhimbili University of Health and Allied Sciences, Dar es Salaam, 65013, Tanzania.
Sci Rep. 2023 Nov 22;13(1):20493. doi: 10.1038/s41598-023-47795-1.
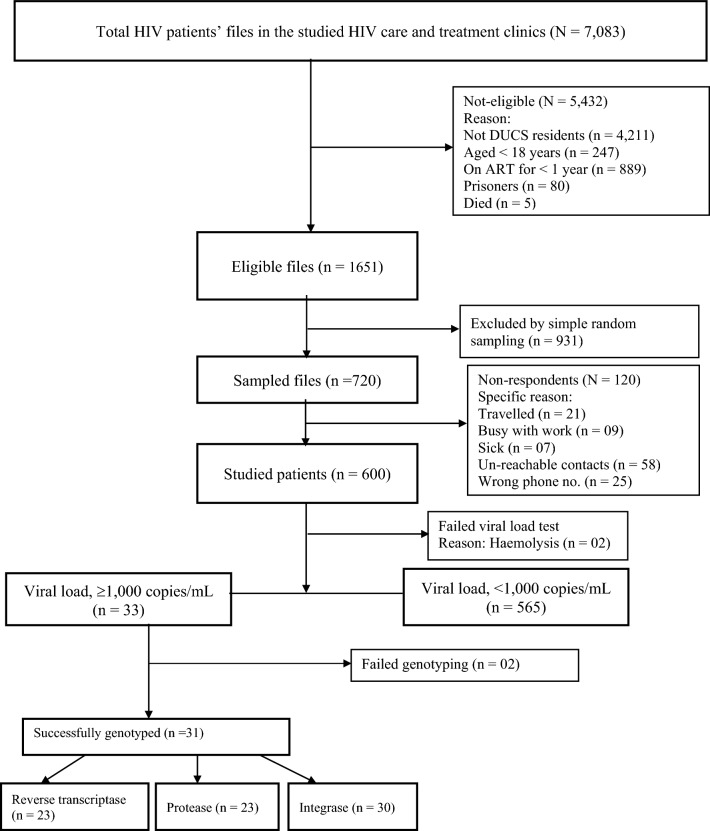
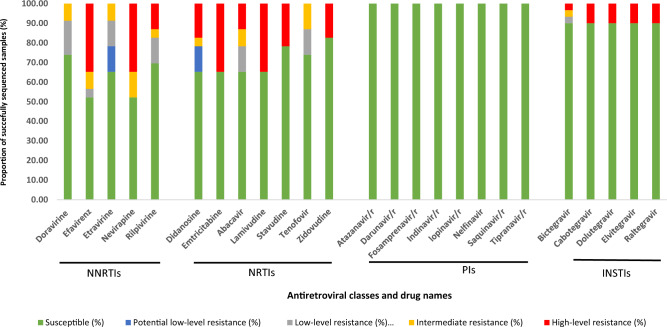
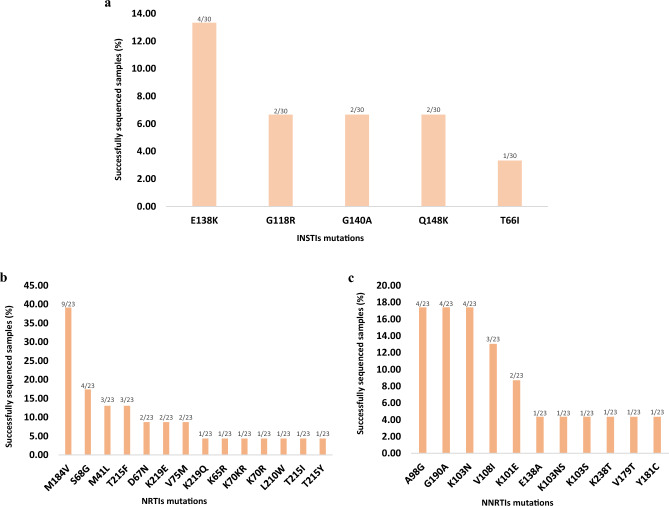
To curb HIV infection rate in Tanzania, antiretroviral therapy (ART) has been scaled up since 2006, and in 2019, the country shifted to regimen including dolutegravir as a default first line. We assessed the success of ART and the contribution of HIV drug resistance (HIVDR) to unsuppressed viral loads. Between February and May 2023 a cross-sectional survey with random sampling was conducted in the six clinics in an urban cohort in Dar es Salaam. Patients with unsuppresed viral loads (local criteria viral load (VL) ≥ 1000 copies/mL) were tested for HIVDR mutations using the WHO adapted protocol for plasma samples. Mutations were interpreted using the Stanford HIVDR database. In total 600 individuals participated in this survey, the majority were female (76.83%), mean age ([Formula: see text] standard deviation) was 44.0 ([Formula: see text] 11.6) years. The median duration on ART (interquartile range) was 6.5 (3.9-10.2) years. Approximately 99% were receiving tenofovir + lamivudine + dolutegravir as a fixed dose combination. VL testing was successful in 99.67% (598/600) of survey patients and only 33 had VL ≥ 1000 copies/mL, resulting in a viral suppression level of 94.48% (565/598, 95% CI 92.34-96.17%). For 23 samples, protease and reverse transcriptase (RT) genotyping were successful, with 13 sequences containing RT inhibitor surveillance drug resistance mutations (SDRMs) (56.5%). No SDRM against protease inhibitors were detected. Thirty samples were successfully genotyped for integrase with 3 sequences (10.08%) containing integrase strand transfer inhibitor (INSTI) SDRMs. In samples successfully genotyped in the three genetic regions, 68.18% (16/22) had a genotypic susceptibility score (GSS) ≥ 2.5 for the concurrent regimen, implying factors beyond drug resistance caused the unsuppressed viral load. For five patients, GSS indicated that HIVDR may have caused the unsuppressed viral load. All three patients with INSTI resistance mutations were highly resistant to dolutegravir and accumulated nucleoside and non-nucleoside RT inhibitor HIVDR mutations. Although in this cohort the last 95 UNAIDS target was almost achieved, HIVDR mutations, including INSTIs resistance mutations were detected in HIV-positive individuals taking ART for at least one year. We recommend the design and implementation of high-impact interventions to prevent the increase of HIVDR, failure of dolutegravir and address the non-resistance factors in the study area.
为了遏制坦桑尼亚的艾滋病毒感染率,自 2006 年以来,抗逆转录病毒疗法(ART)的规模不断扩大,2019 年,该国转向了包含度鲁特韦的方案,作为默认的一线治疗方案。我们评估了 ART 的成功情况以及艾滋病毒耐药性(HIVDR)对未抑制病毒载量的影响。2023 年 2 月至 5 月期间,在达累斯萨拉姆的一个城市队列的六家诊所进行了一项横断面调查,采用随机抽样方法。对未抑制病毒载量(当地标准病毒载量(VL)≥1000 拷贝/mL)的患者使用世卫组织改编的血浆样本 HIVDR 检测协议进行 HIVDR 突变检测。使用斯坦福 HIVDR 数据库对突变进行解释。共有 600 人参加了这项调查,大多数是女性(76.83%),平均年龄([Formula: see text]标准差)为 44.0([Formula: see text]11.6)岁。接受 ART 的中位时间(四分位间距)为 6.5(3.9-10.2)年。大约 99%的患者接受替诺福韦+拉米夫定+度鲁特韦固定剂量复方制剂治疗。VL 检测在 99.67%(598/600)的调查患者中成功进行,只有 33 人 VL≥1000 拷贝/mL,导致病毒抑制率为 94.48%(565/598,95%CI 92.34-96.17%)。对 23 个样本进行了蛋白酶和逆转录酶(RT)基因分型,其中 13 个序列含有 RT 抑制剂监测耐药突变(SDRMs)(56.5%)。未检测到针对蛋白酶抑制剂的 SDRM。对 30 个样本进行了整合酶基因分型,其中 3 个序列(10.08%)含有整合酶链转移抑制剂(INSTI)SDRMs。在三个基因区域成功进行基因分型的样本中,68.18%(16/22)的当前方案的基因型耐药评分(GSS)≥2.5,这表明未抑制病毒载量的原因除了耐药性之外还有其他因素。对于五名患者,GSS 表明 HIVDR 可能导致了未抑制的病毒载量。所有三名携带 INSTI 耐药突变的患者对度鲁特韦高度耐药,并积累了核苷和非核苷逆转录酶抑制剂 HIVDR 突变。尽管在这个队列中,最后一个 UNAIDS 目标几乎实现,但在接受至少一年 ART 治疗的 HIV 阳性个体中,发现了 HIVDR 突变,包括 INSTI 耐药突变。我们建议设计和实施高影响力的干预措施,以防止 HIVDR 的增加、度鲁特韦的失效,并解决研究区域中非耐药因素的问题。