Strizki Julie M, Grobler Jay A, Murgolo Nicholas, Fridman Arthur, Johnson Matthew G, Du Jiejun, Carmelitano Patricia, Brown Michelle L, Paschke Amanda, De Anda Carisa
Merck & Co., Inc., 90 E Scott Ave, Rahway, NJ, 07065, USA.
Infect Dis Ther. 2023 Dec;12(12):2725-2743. doi: 10.1007/s40121-023-00891-1. Epub 2023 Nov 23.
The randomized, placebo-controlled, double-blind MOVe-OUT trial demonstrated molnupiravir (800 mg every 12 h for 5 days) as safe and effective for outpatient treatment of mild-to-moderate COVID-19, significantly reducing the risk of hospitalization/death in high-risk adults. At the time of that report, virologic assessments from the trial were partially incomplete as a result of their time-intensive nature. Here we present final results from all prespecified virology endpoints in MOVe-OUT based on the full trial dataset.
Nasopharyngeal swabs were collected at baseline (day 1, prior to first dose) and days 3, 5 (end-of-treatment visit), 10, 15, and 29. From these samples, change from baseline in SARS-CoV-2 RNA titers (determined by quantitative PCR), detection of infectious SARS-CoV-2 (by plaque assay), and SARS-CoV-2 viral error induction (determined by whole genome next-generation sequencing) were assessed as exploratory endpoints.
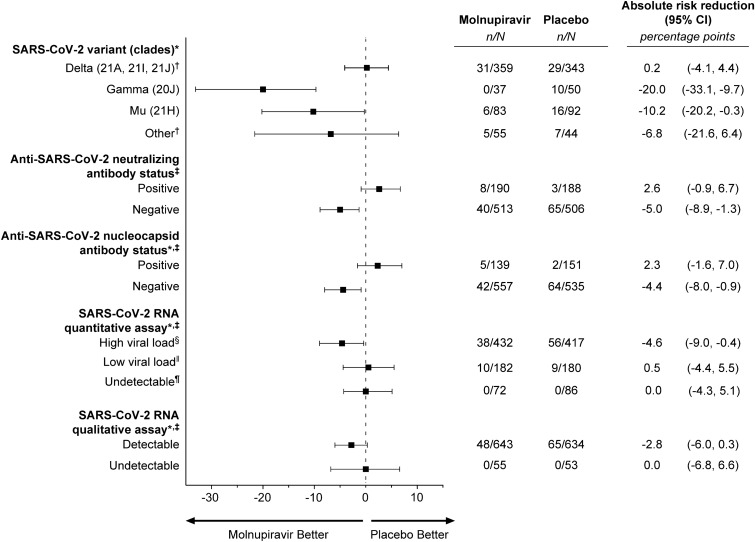
Molnupiravir was associated with greater mean reductions from baseline in SARS-CoV-2 RNA than placebo (including 50% relative reduction at end-of-treatment) through day 10. Among participants with infectious virus detected at baseline (n = 96 molnupiravir, n = 97 placebo) and evaluable post-baseline samples, no molnupiravir-treated participant had infectious SARS-CoV-2 by day 3, whereas infectious virus was recovered from 21% of placebo-arm participants on day 3 and 2% at end-of-treatment. Consistent with molnupiravir's mechanism of action, sequence analysis demonstrated that molnupiravir was associated with an increased number of low-frequency transition errors randomly distributed across the SARS-CoV-2 RNA genome compared with placebo (median 143.5 molnupiravir, 15 placebo), while transversion errors were infrequent overall (median 2 in both arms). Outcomes were consistent regardless of baseline SARS-CoV-2 clade, presence of SARS-CoV-2-specific immune response, or viral load.
A 5-day course of orally administered molnupiravir demonstrated a consistently greater virologic effect than placebo, including rapidly eliminating infectious SARS-CoV-2, in high-risk outpatients with mild-to-moderate COVID-19.
ClinicalTrials.gov, NCT04575597.
随机、安慰剂对照、双盲的MOVe - OUT试验证明,莫努匹拉韦(每12小时800毫克,共5天)对门诊治疗轻至中度COVID - 19安全有效,显著降低了高危成年人住院/死亡风险。在该报告发布时,由于试验中病毒学评估耗时较长,部分评估结果并不完整。在此,我们根据完整试验数据集展示MOVe - OUT试验中所有预先设定的病毒学终点的最终结果。
在基线(第1天,首次给药前)、第3天、第5天(治疗结束访视)、第10天、第15天和第29天采集鼻咽拭子。从这些样本中,评估严重急性呼吸综合征冠状病毒2(SARS-CoV-2)RNA滴度相对于基线的变化(通过定量聚合酶链反应测定)、传染性SARS-CoV-2的检测(通过蚀斑测定)以及SARS-CoV-2病毒错误诱导(通过全基因组下一代测序测定)作为探索性终点。
在第10天之前,莫努匹拉韦组SARS-CoV-2 RNA相对于基线的平均降低幅度大于安慰剂组(包括治疗结束时相对降低50%)。在基线时检测到有传染性病毒的参与者中(莫努匹拉韦组n = 96,安慰剂组n = 97)以及可评估的基线后样本中,到第3天,莫努匹拉韦治疗组没有参与者的SARS-CoV-2具有传染性,而在第3天,安慰剂组21%的参与者病毒仍具有传染性,治疗结束时这一比例为2%。与莫努匹拉韦的作用机制一致,序列分析表明,与安慰剂相比,莫努匹拉韦与随机分布在SARS-CoV-2 RNA基因组中的低频转换错误数量增加有关(莫努匹拉韦组中位数为143.5,安慰剂组为15),而总体上颠换错误很少见(两组中位数均为2)。无论基线SARS-CoV-2进化枝、SARS-CoV-2特异性免疫反应的存在与否或病毒载量如何,结果都是一致的。
对于轻至中度COVID - 19的高危门诊患者,为期5天的口服莫努匹拉韦疗程显示出比安慰剂持续更强的病毒学效应,包括迅速清除传染性SARS-CoV-2。
ClinicalTrials.gov,NCT04575597。