Department of Anesthesiology and Intensive Therapy, Semmelweis University, 1082 Üllői út 78/B, Budapest, Hungary.
Department of Pediatrics, Semmelweis University, Budapest, Hungary.
BMC Pulm Med. 2023 Nov 28;23(1):477. doi: 10.1186/s12890-023-02777-x.
Continuous positive airway pressure (CPAP) therapy has profound effects in obesity hypoventilation syndrome (OHS). Current therapy initiation focuses on upper airway patency rather than the assessment of altered respiratory mechanics due to increased extrapulmonary mechanical load.
We aimed to examine the viability of intra-breath oscillometry in optimizing CPAP therapy for OHS. We performed intra-breath oscillometry at 10 Hz in the sitting and supine positions, followed by measurements at increasing CPAP levels (none-5-10-15-20 cmHO) in awake OHS patients. We plotted intra-breath resistance and reactance (Xrs) values against flow (V') and volume (V) to identify tidal expiratory flow limitation (tEFL).
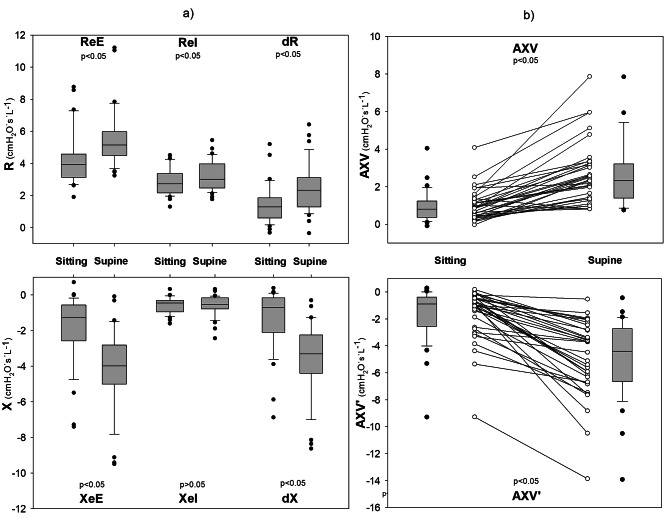
Thirty-five patients (65.7% male) completed the study. We found a characteristic looping of the Xrs vs V' plot in all patients in the supine position revealing tEFL: Xrs fell with decreasing flow at end-expiration. Intra-breath variables representing expiratory decrease of Xrs became more negative in the supine position [end-expiratory Xrs (mean ± SD): -1.9 ± 1.8 cmHO·s·L sitting vs. -4.2 ± 2.2 cmHO·s·L supine; difference between end-expiratory and end-inspiratory Xrs: -1.3 ± 1.7 cmHO·s·L sitting vs. -3.6 ± 2.0 cmHO·s·L supine, p < 0.001]. Increasing CPAP altered expiratory Xrs values and loop areas, suggesting diminished tEFL (p < 0.001). 'Optimal CPAP' value (able to cease tEFL) was 14.8 ± 4.1 cmHO in our cohort, close to the long-term support average of 13.01(± 2.97) cmHO but not correlated. We found no correlation between forced spirometry values, patient characteristics, apnea-hypopnea index and intra-breath oscillometry variables.
tEFL, worsened by the supine position, can be diminished by stepwise CPAP application in most patients. Intra-breath oscillometry is a viable method to detect tEFL during CPAP initiation in OHS patients and tEFL is a possible target for optimizing therapy in OHS patients.
持续气道正压通气(CPAP)治疗对肥胖低通气综合征(OHS)有显著影响。目前的治疗启动侧重于上呼吸道通畅性,而不是由于肺外机械负荷增加而评估呼吸力学的改变。
我们旨在研究呼吸内振荡测量在优化 OHS 的 CPAP 治疗中的可行性。我们在坐位和仰卧位以 10 Hz 进行呼吸内振荡测量,然后在清醒 OHS 患者中在增加的 CPAP 水平(无-5-10-15-20 cmHO)下进行测量。我们将呼吸内阻力和电抗(Xrs)值与流量(V')和体积(V)作图,以确定潮气呼气流量限制(tEFL)。
35 名患者(65.7%为男性)完成了研究。我们发现所有仰卧位患者的 Xrs 与 V' 图都有特征性的环,表明存在 tEFL:Xrs 在呼气末随流量下降而下降。呼吸内变量代表呼气末 Xrs 的下降在仰卧位时变得更加负[呼气末 Xrs(均值±标准差):-1.9±1.8 cmHO·s·L 坐位与-4.2±2.2 cmHO·s·L 仰卧位;呼气末和吸气末 Xrs 之间的差值:-1.3±1.7 cmHO·s·L 坐位与-3.6±2.0 cmHO·s·L 仰卧位,p<0.001]。增加 CPAP 改变了呼气末 Xrs 值和环面积,表明 tEFL 减弱(p<0.001)。我们队列中的“最佳 CPAP”值(能够终止 tEFL)为 14.8±4.1 cmHO,接近长期支持的平均 13.01(±2.97)cmHO,但没有相关性。我们没有发现用力肺活量值、患者特征、呼吸暂停低通气指数和呼吸内振荡测量变量之间的相关性。
在大多数患者中,仰卧位会加重潮气呼气流量限制,通过逐步 CPAP 应用可以减轻这种限制。呼吸内振荡测量是在 OHS 患者中启动 CPAP 治疗时检测 tEFL 的可行方法,tEFL 可能是优化 OHS 患者治疗的目标。