Wisse Pieter H A, de Boer Sybrand Y, Oudkerk Pool Marco, Terhaar Sive Droste Jochim S, Verveer Claudia, Meijer Gerrit A, Dekker Evelien, Spaander Manon C W
Gastroenterology and Hepatology, Erasmus MC, Rotterdam, Netherlands.
Gastroenterology and Hepatology, Bevolkingsonderzoek Nederland, Rotterdam, Netherlands.
Endoscopy. 2024 May;56(5):364-372. doi: 10.1055/a-2230-5563. Epub 2023 Dec 15.
Post-colonoscopy colorectal cancers (PCCRCs) decrease the effect of colorectal cancer (CRC) screening programs. To enable PCCRC incidence reduction in the long-term, we classified PCCRCs diagnosed after colonoscopies performed in a fecal immunochemical test (FIT)-based screening program.
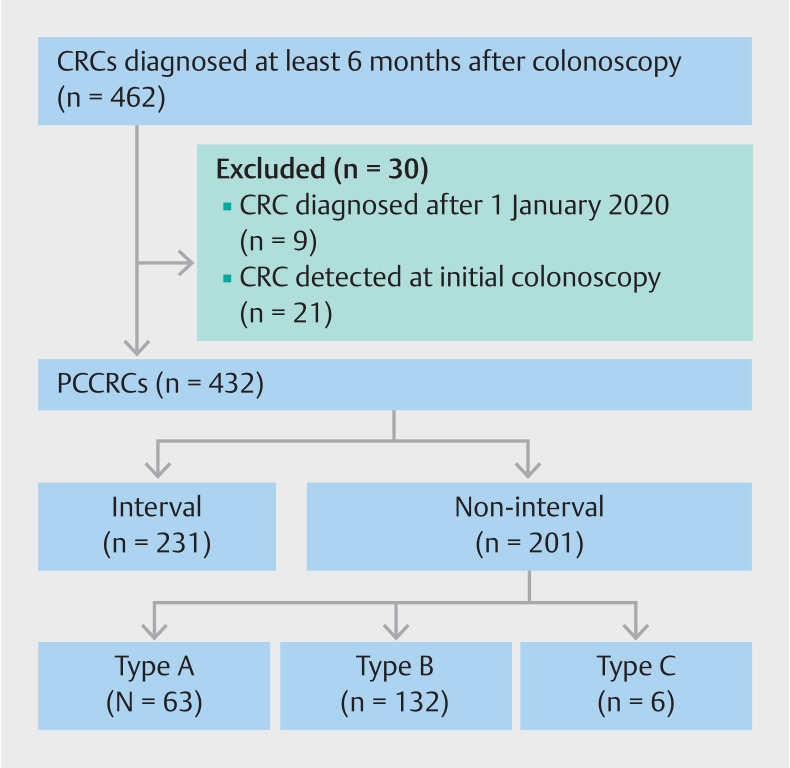
PCCRCs diagnosed after colonoscopies performed between 2014-2016 for a positive FIT in the Dutch CRC screening program were included. PCCRCs were categorized according to the World Endoscopy Organization consensus statement into (a) interval PCCRC (diagnosed before the recommended surveillance); (b) non-interval type A (diagnosed at the recommended surveillance interval); (c) non-interval type B (diagnosed after the recommended surveillance interval); or (d) non-interval type C (diagnosed after the intended recommended surveillance interval, with surveillance not implemented owing to co-morbidity). The most probable etiology was determined by root-cause analysis. Tumor stage distributions were compared between categories.
116362 colonoscopies were performed after a positive FIT with 9978 screen-detected CRCs. During follow-up, 432 PCCRCs were diagnosed. The 3-year PCCRC rate was 2.7%. PCCRCs were categorized as interval (53.5%), non-interval type A (14.6%), non-interval type B (30.6%), and non-interval type C (1.4%). The most common etiology for interval PCCRCs was possible missed lesion with adequate examination (73.6%); they were more often diagnosed at an advanced stage (stage III/IV; 53.2%) compared with non-interval type A (15.9%; <0.001) and non-interval type B (40.9%; =0.03) PCCRCs.
The 3-year PCCRC rate was low in this FIT-based CRC screening program. Approximately half of PCCRCs were interval PCCRCs. These were mostly caused by missed lesions and were diagnosed at a more advanced stage. This emphasizes the importance of high quality colonoscopy with optimal polyp detection.
结肠镜检查后发生的结直肠癌(PCCRC)会降低结直肠癌(CRC)筛查项目的效果。为了长期降低PCCRC的发病率,我们对在基于粪便免疫化学试验(FIT)的筛查项目中结肠镜检查后诊断出的PCCRC进行了分类。
纳入在荷兰CRC筛查项目中因FIT阳性于2014年至2016年间进行结肠镜检查后诊断出的PCCRC。根据世界内镜组织共识声明,将PCCRC分为以下几类:(a)间隔期PCCRC(在推荐的监测时间之前诊断);(b)非间隔期A型(在推荐的监测间隔时诊断);(c)非间隔期B型(在推荐的监测间隔之后诊断);或(d)非间隔期C型(在预期的推荐监测间隔之后诊断,因合并症未实施监测)。通过根本原因分析确定最可能的病因。比较各分类之间的肿瘤分期分布。
FIT阳性后进行了116362例结肠镜检查,其中9978例为筛查发现的CRC。在随访期间,诊断出432例PCCRC。3年PCCRC发生率为2.7%。PCCRC分为间隔期(53.5%)、非间隔期A型(14.6%)、非间隔期B型(30.6%)和非间隔期C型(1.4%)。间隔期PCCRC最常见的病因是检查充分但可能遗漏病变(73.6%);与非间隔期A型(15.9%;<0.001)和非间隔期B型(40.9%;=0.03)PCCRC相比,间隔期PCCRC更常被诊断为晚期(III/IV期;53.2%)。
在这个基于FIT的CRC筛查项目中,3年PCCRC发生率较低。大约一半的PCCRC是间隔期PCCRC。这些大多是由漏诊病变引起的,且诊断时分期更晚。这强调了高质量结肠镜检查及最佳息肉检测的重要性。