Department of Nutrition, Food and Exercise Sciences, Faculty of Health and Medical Sciences, University of Surrey, Guildford, GU2 7XH, UK.
Institute for Global Food Security, School of Biological Sciences, Queen's University Belfast, Northern Ireland, UK.
Eur J Nutr. 2024 Mar;63(2):599-611. doi: 10.1007/s00394-023-03286-7. Epub 2024 Jan 11.
Cow's milk is the primary source of iodine in the UK, but consumption of plant-based milk alternatives (PBMA) is increasing and these products are often not fortified with iodine. We evaluated the impact that replacing current milk consumption with PBMA would have on iodine intake.
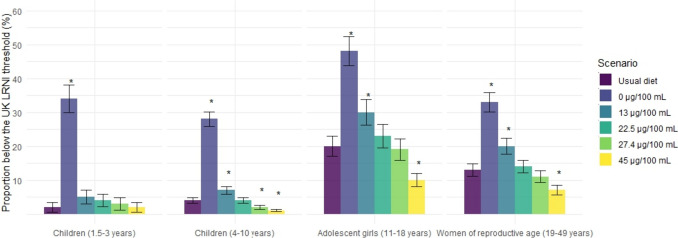
We used data from the National Diet and Nutrition Survey (2016-2019) for children (1.5-10 years), girls 11-18 years, and women of reproductive age (WRA). We used a dietary modelling approach with scenarios using brand-level iodine-fortification data (0, 13, 22.5, 27.4 and 45 µg/100 mL). Relative to usual diet, we calculated change in iodine intake, and the proportion with intake below the Lower Reference Nutrient Intake (LRNI) or above the upper limit.
For all groups, replacement with PBMA, either unfortified or fortified at the lowest concentration, resulted in a meaningful decrease in iodine intake, and increased the proportion with intake < LRNI; compared to usual diet, iodine intake reduced by 58% in children 1.5-3 years (127 vs. 53 µg/day) and the proportion with intake < LRNI increased in girls (11-18 years; 20% to 48%) and WRA (13% to 33%) if an unfortified PBMA was used. Replacement of milk with PBMA fortified at 27.4 µg/100 mL had the lowest impact.
Replacing milk with commercially available PBMAs has potential to reduce population iodine intake, depending on the fortification level. PBMAs fortified with ≥ 22.5 and < 45 µg iodine/100 mL would be required to minimize the impact on iodine intake. Research is needed on the impact of total dairy replacement.
牛奶是英国碘的主要来源,但植物性奶替代品(PBMA)的消费正在增加,而且这些产品通常不添加碘。我们评估了用 PBMA 替代当前牛奶消费对碘摄入量的影响。
我们使用了 2016-2019 年全国饮食和营养调查(National Diet and Nutrition Survey,NDNS)中儿童(1.5-10 岁)、11-18 岁女孩和生育年龄妇女(WRA)的数据。我们使用了一种饮食建模方法,使用品牌层面的碘强化数据(0、13、22.5、27.4 和 45µg/100mL)进行了情景分析。相对于常规饮食,我们计算了碘摄入量的变化,以及摄入量低于下限参考营养素摄入量(Lower Reference Nutrient Intake,LRNI)或高于上限的比例。
对于所有组,用 PBMA 替代,无论是未强化还是以最低浓度强化,都会导致碘摄入量显著下降,并增加摄入量低于 LRNI 的比例;与常规饮食相比,1.5-3 岁儿童的碘摄入量减少了 58%(127 比 53µg/天),女孩(11-18 岁)和 WRA(13%至 33%)的摄入量低于 LRNI 的比例增加,如果使用未强化的 PBMA。用 27.4µg/100mL 强化的 PBMA 替代牛奶的影响最小。
用市售的 PBMA 替代牛奶可能会降低人群的碘摄入量,具体取决于强化水平。需要强化 22.5 至 45µg 碘/100mL 以上的 PBMA,以尽量减少对碘摄入量的影响。需要研究用 PBMA 替代所有乳制品的影响。