Yeo Ilhwan, Axman Rachel, Lu Daniel Y, Feldman Dmitriy N, Cheung Jim W, Minutello Robert M, Karas Maria G, Iannacone Erin M, Srivastava Ankur, Girardi Natalia I, Naka Yoshifumi, Wong Shing-Chiu, Kim Luke K
Division of Cardiology, Department of Medicine, Weill Cornell Medicine New York-Presbyterian Hospital New York NY.
Weill Cornell Cardiovascular Outcomes Research Group (CORG) Weill Cornell Medicine New York NY.
J Am Heart Assoc. 2024 Feb 6;13(3):e032607. doi: 10.1161/JAHA.123.032607. Epub 2024 Jan 19.
Venoarterial extracorporeal membrane oxygenation (VA-ECMO) is increasingly used for patients with cardiogenic shock. Although Impella or intra-aortic balloon pump (IABP) is frequently used for left ventricular unloading (LVU) during VA-ECMO treatment, there are limited data on comparative outcomes. We compared outcomes of Impella and IABP for LVU during VA-ECMO.
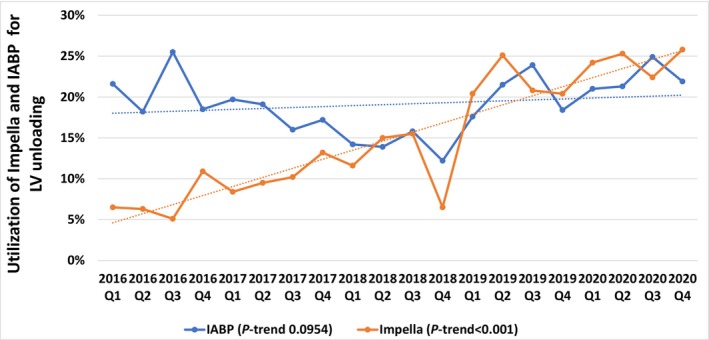
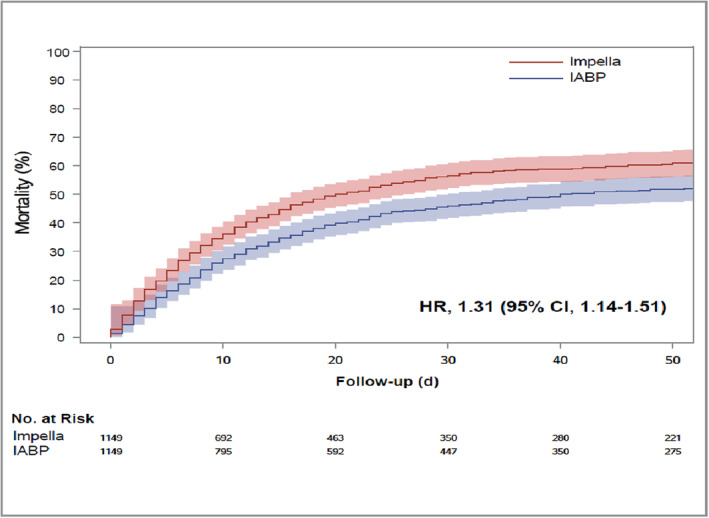
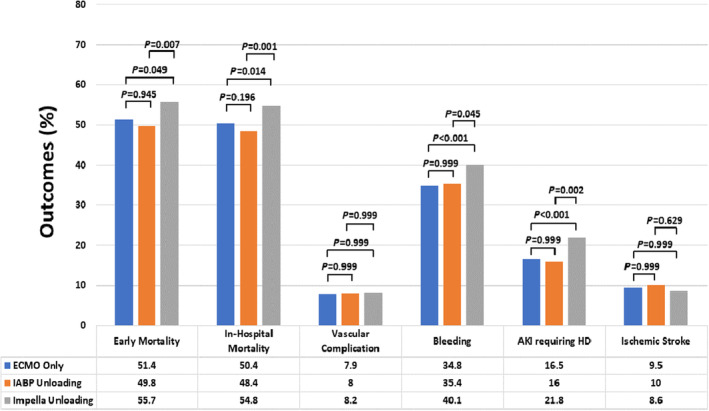
Using the Nationwide Readmissions Database between 2016 and 2020, we analyzed outcomes in 3 groups of patients with cardiogenic shock requiring VA-ECMO based on LVU strategies: extracorporeal membrane oxygenation (ECMO) only, ECMO with IABP, and ECMO with Impella. Of 15 980 patients on VA-ECMO, IABP and Impella were used in 19.4% and 16.4%, respectively. The proportion of patients receiving Impella significantly increased from 2016 to 2020 (6.5% versus 25.8%; -trend<0.001). In-hospital mortality was higher with ECMO with Impella (54.8%) compared with ECMO only (50.4%) and ECMO with IABP (48.4%). After adjustment, ECMO with IABP versus ECMO only was associated with lower in-hospital mortality (adjusted odds ratio [aOR], 0.83; =0.02). ECMO with Impella versus ECMO only had similar in-hospital mortality (aOR, 1.09; =0.695) but was associated with more bleeding (aOR, 1.21; =0.007) and more acute kidney injury requiring hemodialysis (aOR, 1.42; <0.001). ECMO with Impella versus ECMO with IABP was associated with greater risk of acute kidney injury requiring hemodialysis (aOR, 1.49; =0.002), higher in-hospital mortality (aOR, 1.32; =0.001), and higher 40-day mortality (hazard ratio, 1.25; <0.001).
In patients with cardiogenic shock on VA-ECMO, LVU with Impella, particularly with 2.5/CP, was not associated with improved survival at 40 days but was associated with increased adverse events compared with IABP. More data are needed to assess Impella platform-specific comparative outcomes of LVU.
静脉-动脉体外膜肺氧合(VA-ECMO)越来越多地用于心源性休克患者。尽管在VA-ECMO治疗期间经常使用Impella或主动脉内球囊泵(IABP)进行左心室卸载(LVU),但关于比较结果的数据有限。我们比较了VA-ECMO期间使用Impella和IABP进行LVU的结果。
利用2016年至2020年的全国再入院数据库,我们分析了3组需要VA-ECMO的心源性休克患者基于LVU策略的结果:仅体外膜肺氧合(ECMO)、ECMO联合IABP以及ECMO联合Impella。在15980例接受VA-ECMO的患者中,分别有19.4%和16.4%使用了IABP和Impella。从2016年到2020年,接受Impella的患者比例显著增加(6.5%对25.8%;趋势P<0.001)。与仅使用ECMO(50.4%)和ECMO联合IABP(48.4%)相比,ECMO联合Impella的住院死亡率更高(54.8%)。调整后,ECMO联合IABP与仅使用ECMO相比,住院死亡率较低(调整后的优势比[aOR],0.83;P=0.02)。ECMO联合Impella与仅使用ECMO相比,住院死亡率相似(aOR,1.09;P=0.695),但与更多出血(aOR,1.21;P=0.007)和更多需要血液透析的急性肾损伤相关(aOR,1.42;P<0.001)。ECMO联合Impella与ECMO联合IABP相比,需要血液透析的急性肾损伤风险更高(aOR,1.49;P=0.002),住院死亡率更高(aOR,1.32;P=0.001),40天死亡率更高(风险比,1.25;P<0.001)。
在接受VA-ECMO的心源性休克患者中,与IABP相比,使用Impella进行LVU,尤其是使用2.5/CP,在40天时并未改善生存率,但与不良事件增加相关。需要更多数据来评估Impella平台特定的LVU比较结果。