Department of Cardiovascular Surgery, Toyohashi Heart Center, 21-1 Gobudori, Oyama-Cho, Toyohashi, 441-8530, Japan.
J Cardiothorac Surg. 2024 Jan 22;19(1):15. doi: 10.1186/s13019-024-02484-6.
Acute type A aortic dissection is treated with an emergency procedure that uses ascending aortic replacement (AAR). However, to avoid a residual dissected aorta with a false lumen, total arch replacement (TAR) is required. The frozen elephant trunk (FET) technique is a promising surgical approach that promotes false lumen obliteration in a single step. Therefore, this retrospective single-center study aimed to evaluate the operative outcomes of AAR and TAR with FET.
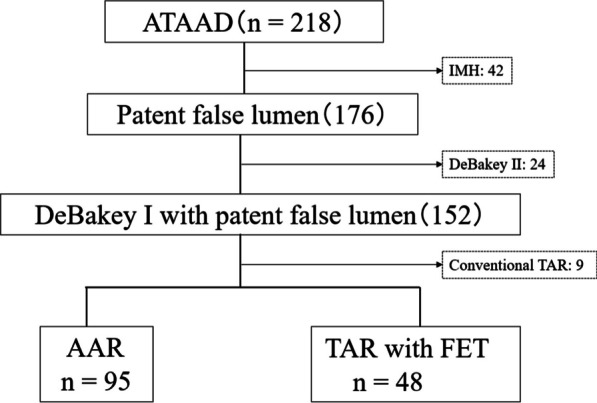
Between 2007 and 2021, 143 patients with acute DeBakey type I aortic dissection underwent a central repair using AAR (n = 95) or TAR with FET (n = 43). All perioperative variables, the duration of all-cause mortality, and aortic events defined as dilatation of the distal aorta > 5 cm, new occurrences of aortic dissection, distal aortic surgery, and distal aortic rupture were recorded. We compared these perioperative variables and mid-term results with an additional focus on distal aortic events.
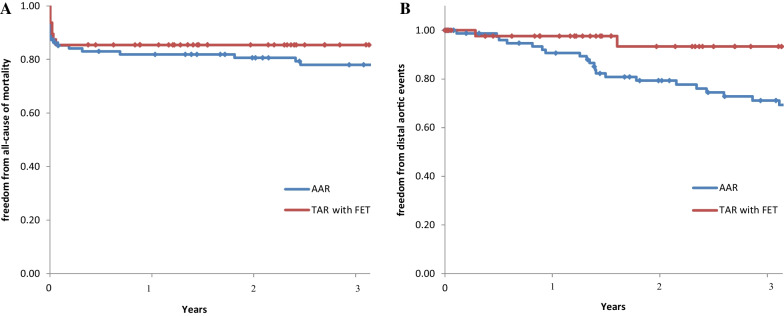
Patient background data did not differ between the two groups. Perioperative results for the TAR with FET group vs the AAR group showed similar operative times (306 vs 298 min, P = 0.862), but the TAR group had longer cardiopulmonary bypass times (154 vs 179 min, P < 0.001). The freedom from all-cause death for the TAR vs AAR groups using the Kaplan-Meier method was 81.9% vs 85.4% and 78.0% vs 85.4% (P = 0.407) at 1 and 3 years, respectively. Freedom from aorta-related events was 90.6% vs 97.6% and 69.3% vs 87.0% (P = 0.034) at 1 and 3 years, respectively.
TAR with FET had comparable perioperative results to AAR in acute DeBakey type I aortic dissection and was considered a valuable method to avoid aorta-related events in the midterm.
急性A型主动脉夹层采用急诊手术治疗,使用升主动脉置换术(AAR)。然而,为了避免假腔存在残留的主动脉夹层,需要进行全主动脉弓置换术(TAR)。冷冻象鼻技术(FET)是一种有前途的手术方法,可在一步中促进假腔闭塞。因此,本回顾性单中心研究旨在评估 AAR 和 TAR 联合 FET 的手术结果。
2007 年至 2021 年间,143 例急性 DeBakey I 型主动脉夹层患者接受了中心修复手术,其中 95 例行 AAR,43 例行 TAR 联合 FET。记录所有围手术期变量、全因死亡率持续时间以及主动脉事件(定义为远端主动脉扩张>5cm、新发主动脉夹层、远端主动脉手术和远端主动脉破裂)。我们比较了这些围手术期变量和中期结果,并特别关注了远端主动脉事件。
两组患者的背景数据无差异。TAR 联合 FET 组与 AAR 组的围手术期结果显示手术时间相似(306 分钟 vs. 298 分钟,P=0.862),但 TAR 组体外循环时间更长(154 分钟 vs. 179 分钟,P<0.001)。TAR 组与 AAR 组患者的全因死亡无事件生存率分别为 81.9%和 85.4%,Kaplan-Meier 法计算的 1 年和 3 年分别为 78.0%和 85.4%(P=0.407)。主动脉相关事件无事件生存率分别为 90.6%和 97.6%,Kaplan-Meier 法计算的 1 年和 3 年分别为 69.3%和 87.0%(P=0.034)。
TAR 联合 FET 在急性 DeBakey I 型主动脉夹层中的围手术期结果与 AAR 相当,是一种在中期避免主动脉相关事件的有价值方法。