Reznichenko Anna, Nair Viji, Eddy Sean, Fermin Damian, Tomilo Mark, Slidel Timothy, Ju Wenjun, Henry Ian, Badal Shawn S, Wesley Johnna D, Liles John T, Moosmang Sven, Williams Julie M, Quinn Carol Moreno, Bitzer Markus, Hodgin Jeffrey B, Barisoni Laura, Karihaloo Anil, Breyer Matthew D, Duffin Kevin L, Patel Uptal D, Magnone Maria Chiara, Bhat Ratan, Kretzler Matthias
Translational Science & Experimental Medicine, Research and Early Development, Cardiovascular, Renal and Metabolism, BioPharmaceuticals R&D, AstraZeneca, Gothenburg, Sweden.
Department of Internal Medicine, Division of Nephrology, University of Michigan, Ann Arbor, Michigan, USA.
Kidney Int. 2024 Jun;105(6):1263-1278. doi: 10.1016/j.kint.2024.01.012. Epub 2024 Jan 27.
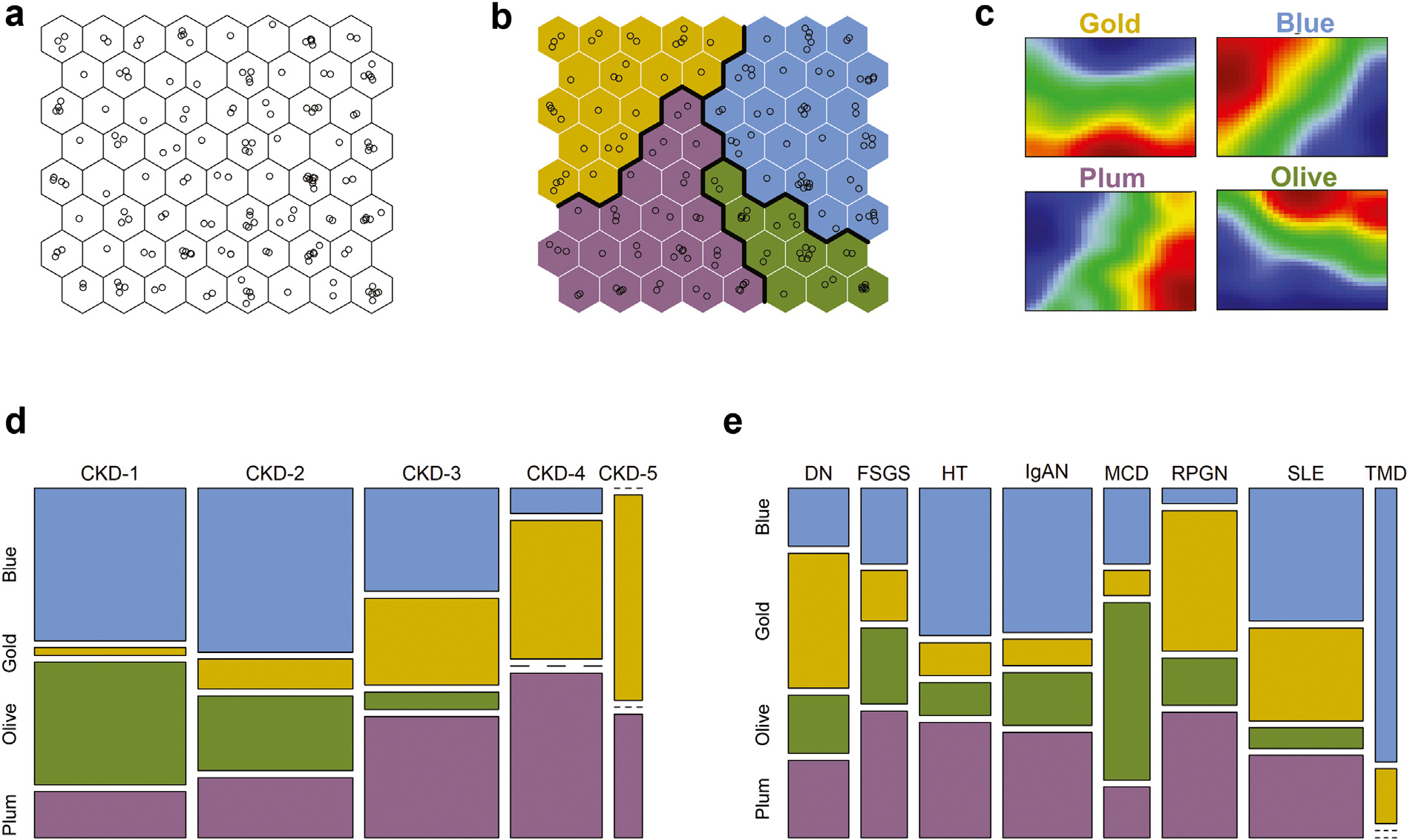
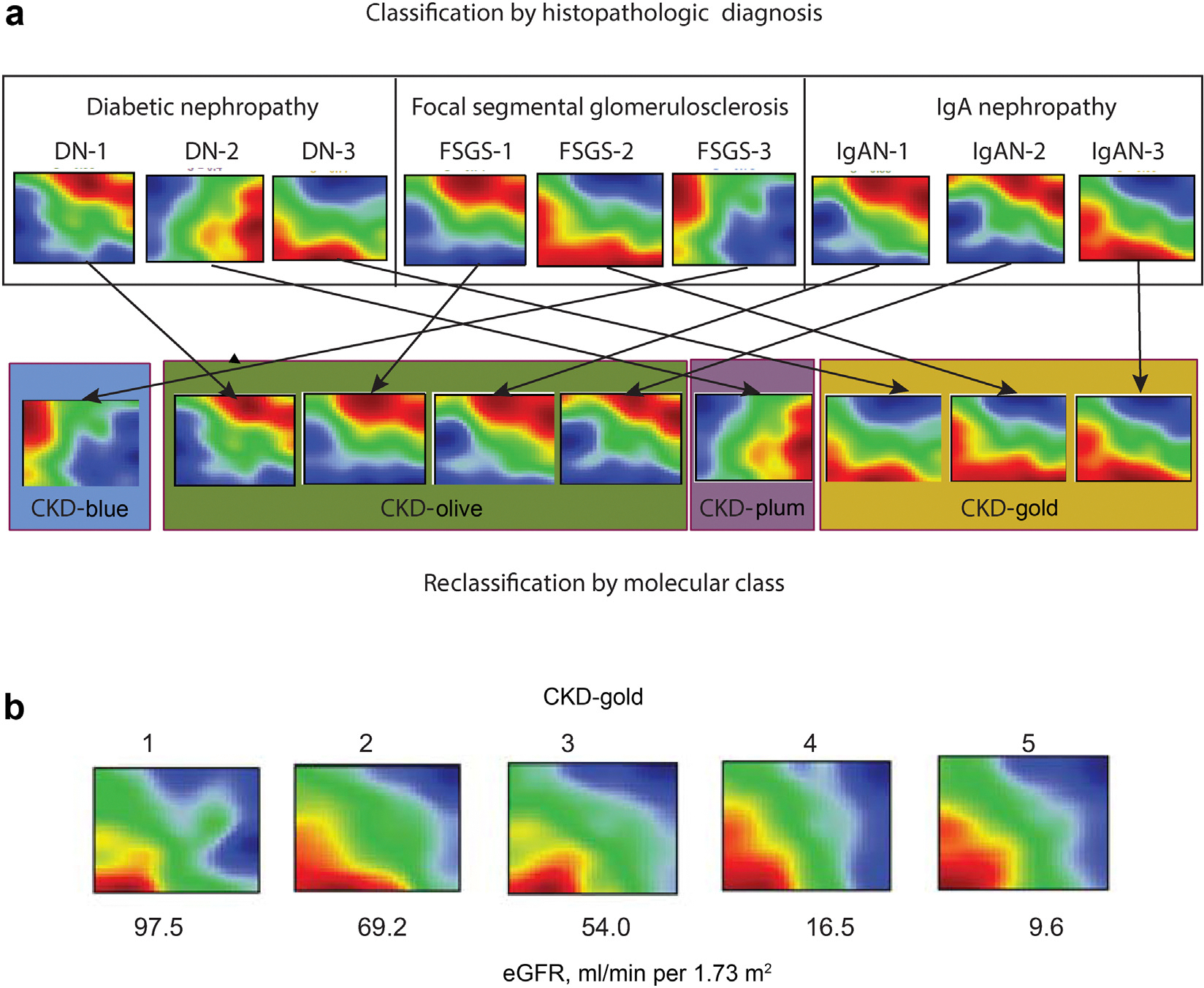
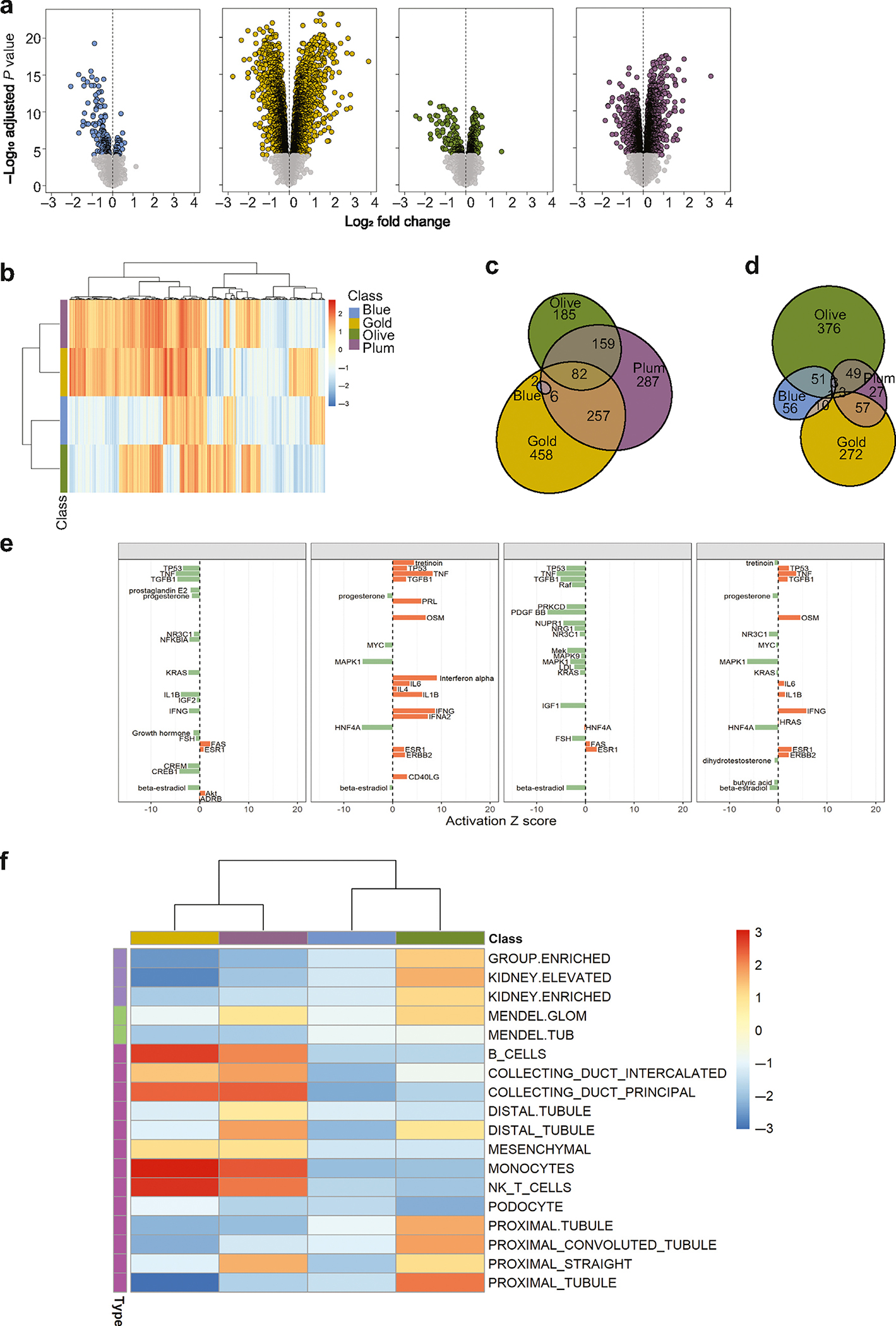
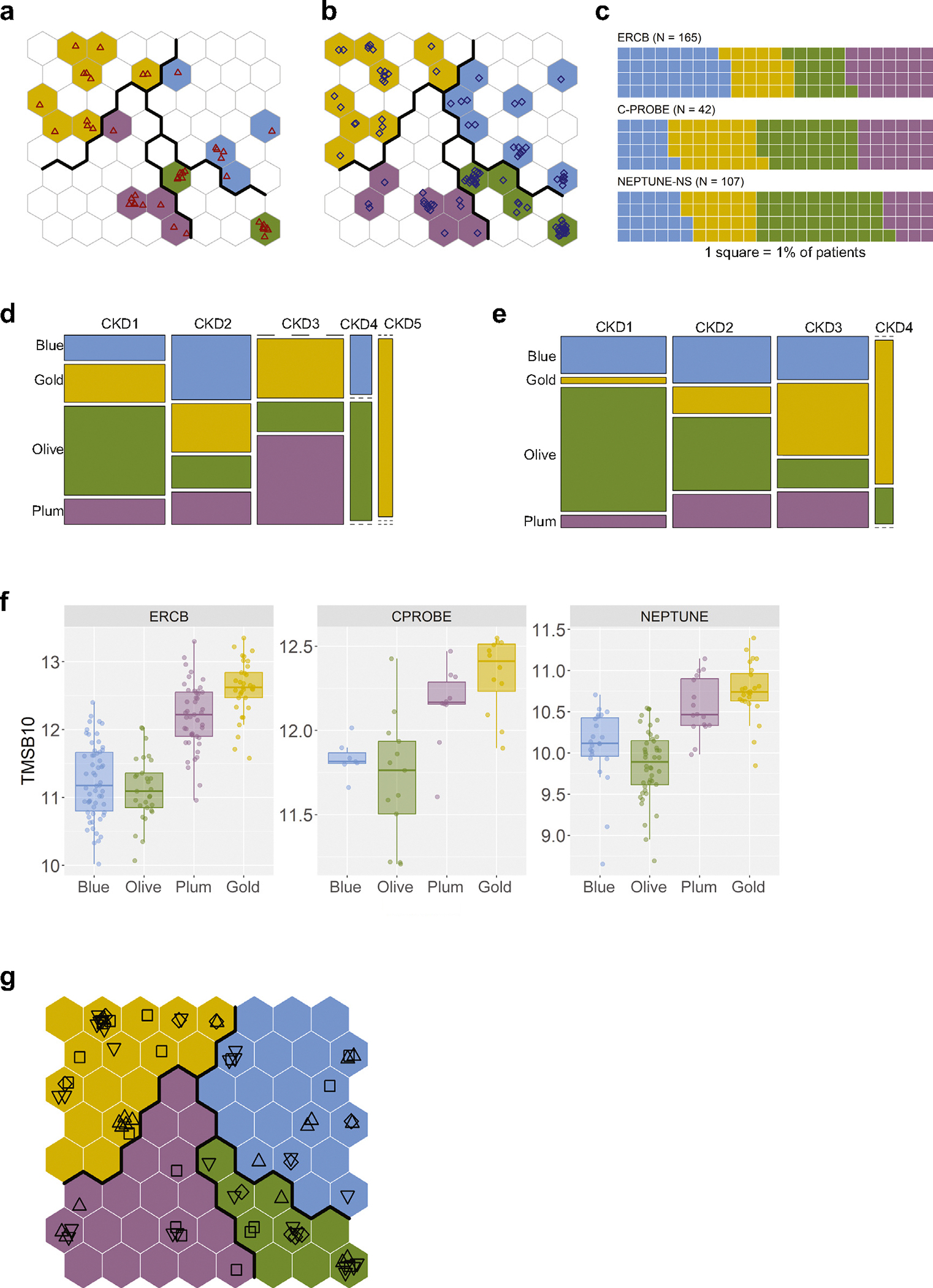
Current classification of chronic kidney disease (CKD) into stages using indirect systemic measures (estimated glomerular filtration rate (eGFR) and albuminuria) is agnostic to the heterogeneity of underlying molecular processes in the kidney thereby limiting precision medicine approaches. To generate a novel CKD categorization that directly reflects within kidney disease drivers we analyzed publicly available transcriptomic data from kidney biopsy tissue. A Self-Organizing Maps unsupervised artificial neural network machine-learning algorithm was used to stratify a total of 369 patients with CKD and 46 living kidney donors as healthy controls. Unbiased stratification of the discovery cohort resulted in identification of four novel molecular categories of disease termed CKD-Blue, CKD-Gold, CKD-Olive, CKD-Plum that were replicated in independent CKD and diabetic kidney disease datasets and can be further tested on any external data at kidneyclass.org. Each molecular category spanned across CKD stages and histopathological diagnoses and represented transcriptional activation of distinct biological pathways. Disease progression rates were highly significantly different between the molecular categories. CKD-Gold displayed rapid progression, with significant eGFR-adjusted Cox regression hazard ratio of 5.6 [1.01-31.3] for kidney failure and hazard ratio of 4.7 [1.3-16.5] for composite of kidney failure or a 40% or more eGFR decline. Urine proteomics revealed distinct patterns between the molecular categories, and a 25-protein signature was identified to distinguish CKD-Gold from other molecular categories. Thus, patient stratification based on kidney tissue omics offers a gateway to non-invasive biomarker-driven categorization and the potential for future clinical implementation, as a key step towards precision medicine in CKD.
目前使用间接全身指标(估计肾小球滤过率(eGFR)和蛋白尿)将慢性肾脏病(CKD)分为不同阶段的方法,无法识别肾脏潜在分子过程的异质性,从而限制了精准医学方法的应用。为了生成一种直接反映肾脏疾病驱动因素的新型CKD分类方法,我们分析了来自肾活检组织的公开转录组数据。使用自组织映射无监督人工神经网络机器学习算法,将总共369例CKD患者和46例活体肾供体作为健康对照进行分层。对发现队列的无偏分层导致识别出四种新型疾病分子类别,称为CKD-蓝色、CKD-金色、CKD-橄榄色、CKD-李子色,这些类别在独立的CKD和糖尿病肾病数据集中得到了重复,并且可以在kidneyclass.org上的任何外部数据上进一步测试。每个分子类别跨越CKD阶段和组织病理学诊断,并代表不同生物途径的转录激活。分子类别之间的疾病进展率差异非常显著。CKD-金色显示出快速进展,肾衰竭的eGFR校正Cox回归风险比为5.6[1.01-31.3],肾衰竭或eGFR下降40%或更多的复合终点风险比为4.7[1.3-16.5]。尿液蛋白质组学揭示了分子类别之间的不同模式,并确定了一个25蛋白特征来区分CKD-金色与其他分子类别。因此,基于肾脏组织组学的患者分层为非侵入性生物标志物驱动的分类提供了途径,并具有未来临床应用的潜力,这是CKD精准医学的关键一步。