Infectious Diseases Service, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland.
Department of Cardiology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland.
Clin Infect Dis. 2024 Apr 10;78(4):949-955. doi: 10.1093/cid/ciae039.
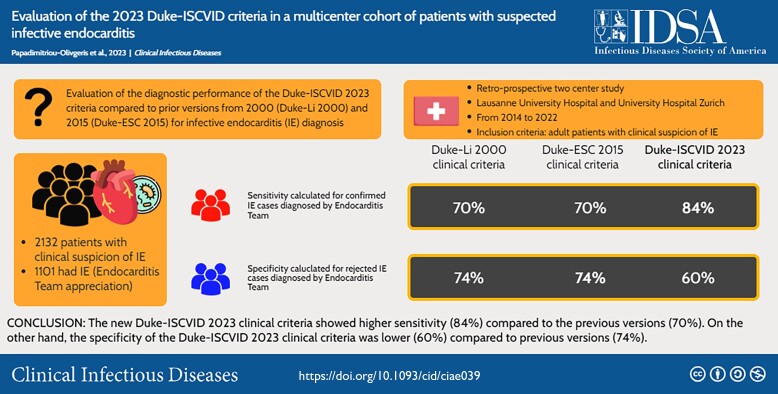
Since publication of Duke criteria for infective endocarditis (IE) diagnosis, several modifications have been proposed. We aimed to evaluate the diagnostic performance of the Duke-ISCVID (International Society of Cardiovascular Infectious Diseases) 2023 criteria compared to prior versions from 2000 (Duke-Li 2000) and 2015 (Duke-ESC [European Society for Cardiology] 2015).
This study was conducted at 2 university hospitals between 2014 and 2022 among patients with suspected IE. A case was classified as IE (final IE diagnosis) by the Endocarditis Team. Sensitivity for each version of the Duke criteria was calculated among patients with confirmed IE based on pathological, surgical, and microbiological data. Specificity for each version of the Duke criteria was calculated among patients with suspected IE for whom IE diagnosis was ruled out.
In total, 2132 episodes with suspected IE were included, of which 1101 (52%) had final IE diagnosis. Definite IE by pathologic criteria was found in 285 (13%), 285 (13%), and 345 (16%) patients using the Duke-Li 2000, Duke-ESC 2015, or the Duke-ISCVID 2023 criteria, respectively. IE was excluded by histopathology in 25 (1%) patients. The Duke-ISCVID 2023 clinical criteria showed a higher sensitivity (84%) compared to previous versions (70%). However, specificity of the new clinical criteria was lower (60%) compared to previous versions (74%).
The Duke-ISCVID 2023 criteria led to an increase in sensitivity compared to previous versions. Further studies are needed to evaluate items that could increase sensitivity by reducing the number of IE patients misclassified as possible, but without having detrimental effect on specificity of Duke criteria.
自杜克感染性心内膜炎(IE)诊断标准发表以来,已经提出了几项修改建议。我们旨在评估 2023 年杜克-ISCVID(国际心血管感染疾病学会)标准与 2000 年(杜克-李 2000 年)和 2015 年(杜克-ESC [欧洲心脏病学会] 2015 年)的前版本相比的诊断性能。
这项研究于 2014 年至 2022 年在两家大学医院进行,对象为疑似 IE 患者。由心内膜炎团队对疑似 IE 患者进行分类。根据病理、手术和微生物学数据,计算每种杜克标准版本在确诊 IE 患者中的敏感性。计算每种杜克标准版本在疑似 IE 患者中的特异性,这些患者排除了 IE 诊断。
共纳入 2132 例疑似 IE 患者,其中 1101 例(52%)最终确诊为 IE。使用杜克-李 2000 年、杜克-ESC 2015 年或杜克-ISCVID 2023 年标准,分别有 285 例(13%)、285 例(13%)和 345 例(16%)患者的病理标准确诊为明确 IE。25 例(1%)患者的组织病理学排除了 IE。与前几个版本相比,2023 年杜克临床标准的敏感性更高(84%)。然而,新的临床标准的特异性较低(60%),低于前几个版本(74%)。
与前几个版本相比,2023 年杜克标准的敏感性有所提高。需要进一步研究评估能够提高敏感性的项目,同时减少被错误分类为可能的 IE 患者数量,而不会对杜克标准的特异性产生不利影响。