Population Data Science, Swansea University Medical School, Faculty of Medicine, Health & Life Science, Swansea University, Swansea, Wales.
NHS Wales Executive, Wales Cardiovascular Network, Cardiff, Wales.
PLoS One. 2024 Feb 9;19(2):e0297049. doi: 10.1371/journal.pone.0297049. eCollection 2024.
The study aimed to assess if specialised healthcare service interventions in Wales benefit the population equitably in work commissioned by the Welsh Health Specialised Services Committee (WHSSC).
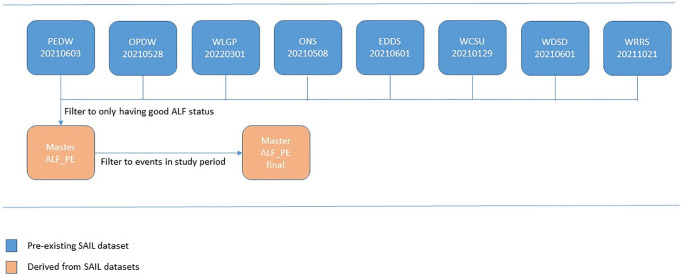
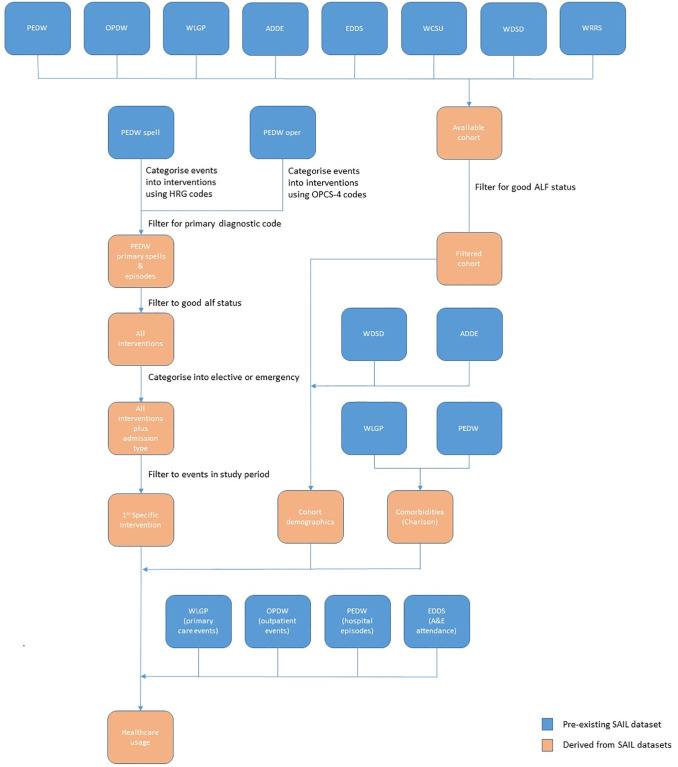
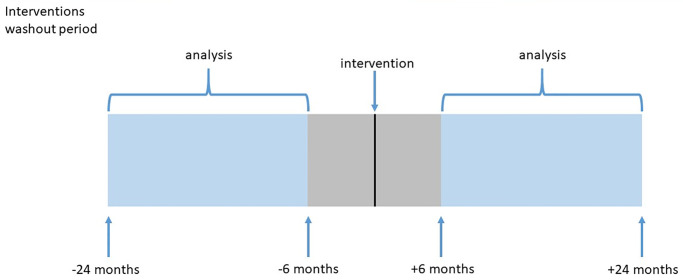
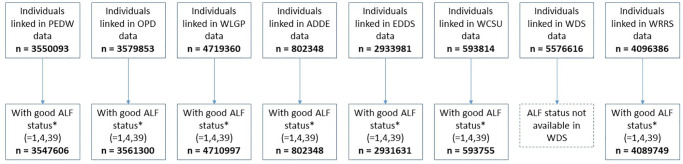
The study utilised anonymised individual-level, population-scale, routinely collected electronic health record (EHR) data held in the Secure Anonymised Information Linkage (SAIL) Databank to identify patients resident in Wales receiving specialist cardiac interventions. Measurement was undertaken of associated patient outcomes 2-years before and after the intervention (minus a 6-month clearance period on either side) by measuring events in primary care, hospital attendance, outpatient and emergency department. The analysis controlled for comorbidity (Charlson) and deprivation (Welsh Index of Multiple Deprivation), stratified by admission type (elective or emergency) and membership of top 5% post-intervention costs. Costs were estimated by multiplying events by mean person cost estimates.
We identified 5,999 percutaneous coronary interventions (PCI) and 1,640 coronary artery bypass graft (CABG) between 2014-06-01 to 2020-02-29. The ratio of emergency to elective interventions was 2.85 for PCI and 1.04 for CABG. In multivariate analysis significant associations were identified for comorbidity (OR = 1.52, CI = (1.01-2.27)), deprivation (OR = 1.34, CI = (1.03-1.76)) and rurality (OR = 0.81, CI = (0.70-0.95)) for PCI interventions, and comorbidity (OR = 1.47, CI = (1.10-1.98)) for CABG. Higher costs post-intervention were associated with increased comorbidity for PCI and CABG in the top 5% cost groups, but for PCI this was not seen outside the top 5%. For PCI, moderate cost increase was associated with increased deprivation, but the picture was more mixed following CABG interventions. For both interventions, lower costs post intervention were seen in rural locations.
We identified and compared health outcomes for selected specialist cardiac interventions amongst patients resident in Wales, with these methods and analyses, providing a template for comparing other cardiac interventions.
本研究旨在评估威尔士的专业医疗保健服务干预措施是否使该地区的人群在威尔士卫生专门服务委员会(WHSSC)委托的工作中受益公平。
本研究利用匿名的、基于人群的、常规收集的电子健康记录(EHR)数据,这些数据保存在安全匿名信息链接(SAIL)数据库中,以确定居住在威尔士的接受心脏专科干预的患者。通过测量初级保健、医院就诊、门诊和急诊部门的事件,在干预前 2 年和干预后(每侧 6 个月的清除期除外)对相关患者结果进行了测量。分析通过控制合并症(Charlson)和贫困(威尔士多重剥夺指数),并按入院类型(选择性或紧急性)和干预后前 5%的成本会员资格进行分层,对事件进行了控制。通过将事件乘以人均成本估算值来估算成本。
我们确定了 2014 年 6 月 1 日至 2020 年 2 月 29 日期间的 5999 例经皮冠状动脉介入治疗(PCI)和 1640 例冠状动脉旁路移植术(CABG)。PCI 的急诊与择期干预之比为 2.85,CABG 的急诊与择期干预之比为 1.04。多变量分析确定了 PCI 干预的合并症(OR = 1.52,CI =(1.01-2.27))、贫困(OR = 1.34,CI =(1.03-1.76))和农村地区(OR = 0.81,CI =(0.70-0.95))之间存在显著关联,CABG 的合并症(OR = 1.47,CI =(1.10-1.98))。在 PCI 和 CABG 的前 5%成本组中,较高的术后并发症与较高的术后并发症相关,但在 PCI 中,在 5%以上则没有发现这种情况。对于 PCI,较高的术后并发症与较高的贫困相关,但 CABG 干预后的情况更为复杂。对于两种干预措施,农村地区的术后成本较低。
我们使用这些方法和分析,确定并比较了居住在威尔士的患者接受选定的心脏专科干预后的健康结果,为比较其他心脏干预措施提供了模板。