Department of Radiation Oncology, Peter MacCallum Cancer Centre, Melbourne, Australia.
Sir Peter MacCallum Department of Oncology, University of Melbourne, Melbourne, Australia.
Radiat Oncol. 2024 Feb 15;19(1):23. doi: 10.1186/s13014-024-02413-w.
Stereotactic ablative body radiotherapy (SABR) is an emerging treatment for patients with primary renal cell carcinoma (RCC). However, its impact on renal function is unclear. This study aimed to evaluate incidence and clinical factors predictive of severe to end-stage chronic kidney disease (CKD) after SABR for RCC.
This was a Single institutional retrospective analysis of patients with diagnosed primary RCC receiving SABR between 2012-2020. Adult patients with no metastatic disease, baseline estimated glomerular filtration rate (eGFR) of ≥ 30 ml/min/1.73 m, and at least one post-SABR eGFR at six months or later were included in this analysis. Patients with upper tract urothelial carcinoma were excluded. Primary outcome was freedom from severe to end-stage CKD, determined using the Kaplan-Meier estimator. The impact of baseline CKD, age, hypertension, diabetes, tumor size and fractionation schedule were assessed by Cox proportional hazard models.
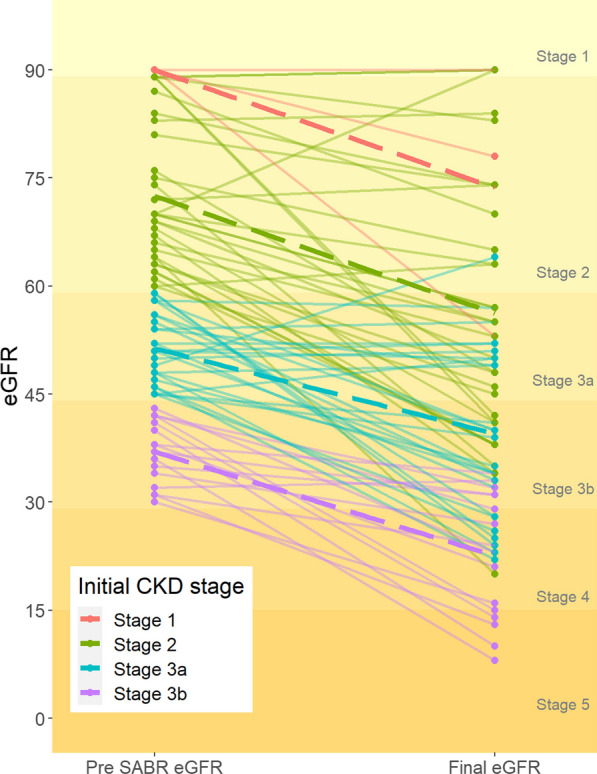
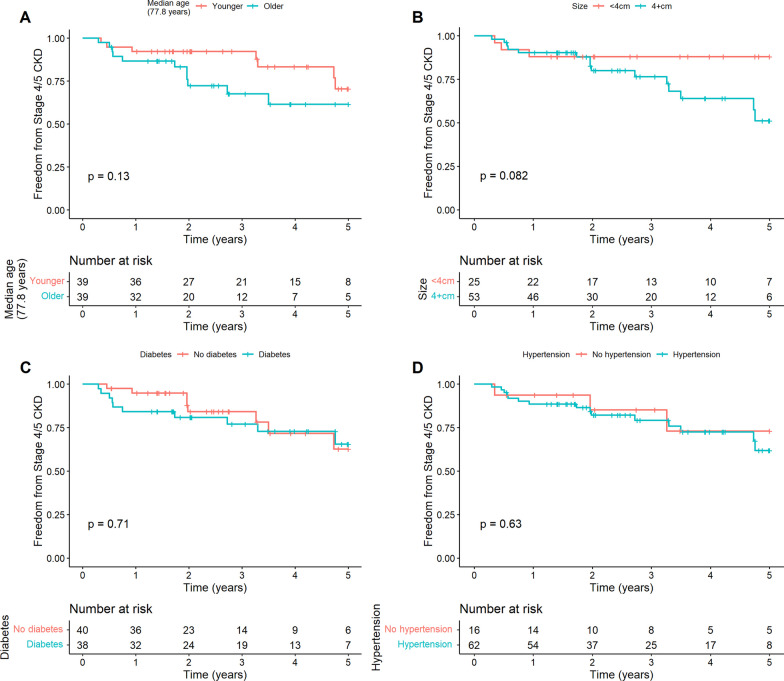
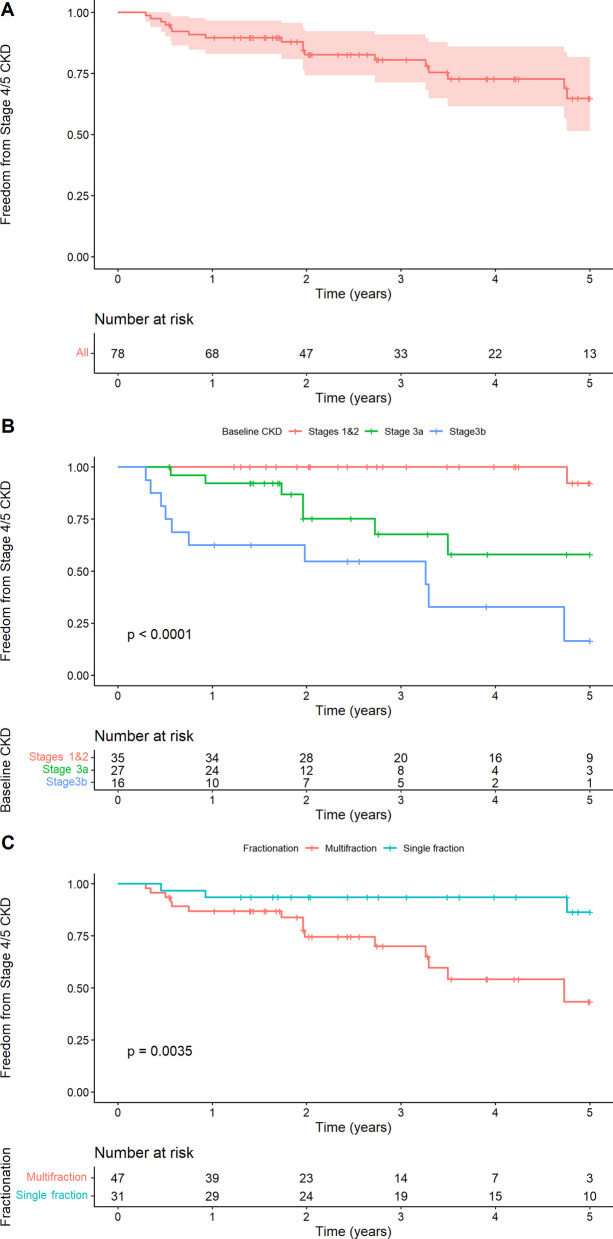
Seventy-eight consecutive patients were included, with median age of 77.8 years (IQR 70-83), tumor size of 4.5 cm (IQR 3.9-5.8) and follow-up of 42.2 months (IQR 23-60). Baseline median eGFR was 58 mls/min; 55% (n = 43) of patients had baseline CKD stage 3 and the remainder stage 1-2. By last follow-up, 1/35 (2.8%) of baseline CKD 1-2, 7/27 (25.9%) CKD 3a and 11/16 (68.8%) CKD 3b had developed CKD stage 4-5. The estimated probability of freedom from CKD stage 4-5 at 1 and 5 years was 89.6% (CI 83.0-97.6) and 65% (CI 51.4-81.7) respectively. On univariable analysis, worse baseline CKD (p < 0.0001) and multi-fraction SABR (p = 0.005) were predictive for development of stage 4-5 CKD though only the former remained significant in multivariable model.
In this elderly cohort with pre-existing renal dysfunction, SABR achieved satisfactory nephron sparing with acceptable rates of severe to end-stage CKD. It can be an attractive option in patients who are medically inoperable.
立体定向消融体放射治疗(SABR)是一种治疗原发性肾癌(RCC)的新兴治疗方法。然而,其对肾功能的影响尚不清楚。本研究旨在评估 SABR 治疗 RCC 后发生严重至终末期慢性肾脏病(CKD)的发生率和临床预测因素。
这是一项单机构回顾性分析,纳入了 2012-2020 年间接受 SABR 治疗的原发性 RCC 患者。纳入标准为:无远处转移疾病、基线估算肾小球滤过率(eGFR)≥30ml/min/1.73m2,且至少有一次 SABR 后 6 个月或以上的 eGFR。排除上尿路尿路上皮癌患者。本研究的主要结局是使用 Kaplan-Meier 估计器评估严重至终末期 CKD 的无病生存率。通过 Cox 比例风险模型评估基线 CKD、年龄、高血压、糖尿病、肿瘤大小和分割方案的影响。
共纳入 78 例连续患者,中位年龄为 77.8 岁(IQR 70-83),肿瘤大小为 4.5cm(IQR 3.9-5.8),随访时间为 42.2 个月(IQR 23-60)。基线中位 eGFR 为 58ml/min;55%(n=43)的患者基线 CKD 分期为 3 期,其余为 1-2 期。末次随访时,35 例基线 CKD 1-2 期患者中,有 1 例(2.8%)、27 例 CKD 3a 期患者中有 7 例(25.9%)和 16 例 CKD 3b 期患者中有 11 例(68.8%)进展为 CKD 4-5 期。1 年和 5 年时无 CKD 4-5 期的估计概率分别为 89.6%(CI 83.0-97.6)和 65%(CI 51.4-81.7)。单变量分析显示,基线 CKD 较差(p<0.0001)和多分割 SABR(p=0.005)是发生 CKD 4-5 期的预测因素,但只有前者在多变量模型中仍有意义。
在本研究中,对于存在肾功障碍的老年患者,SABR 实现了满意的保肾效果,严重至终末期 CKD 的发生率可接受。对于不能手术的患者,SABR 是一种有吸引力的治疗选择。