Department of Internal Medicine, Division of Gastroenterology and Hepatology, Stanford University, Stanford, CA, USA.
Department of Anesthesiology, Perioperative and Pain Medicine, Stanford University, Stanford, CA, USA.
Am J Case Rep. 2024 Feb 15;25:e942906. doi: 10.12659/AJCR.942906.
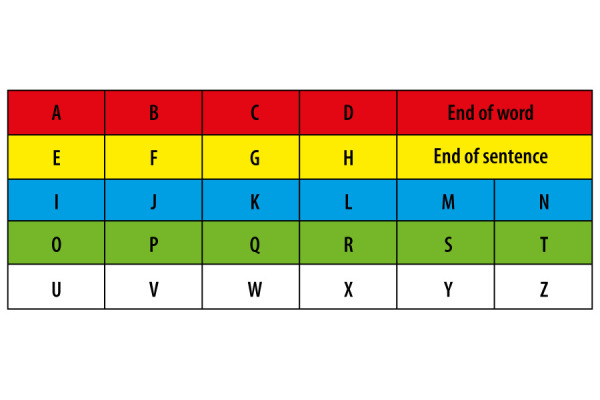
BACKGROUND Delivering safe anesthetic care to a patient unable to communicate easily and effectively with the anesthesia team presents many unique challenges. Communication may be limited by language, which can be resolved with translation services, or neurological conditions, such as stroke or traumatic brain injury, which are not easily remedied. In such patients, the inability to communicate effectively can lead to anxiety and negatively impact the patient-anesthesiologist relationship, especially when higher cognitive functions are preserved. CASE REPORT We present a case of a patient with locked-in syndrome (LIS), who presented to our endoscopy unit for a routine colonoscopy. The patient could only communicate with eye movements and blinking, thus limiting our ability to assess their pain or other needs in the perioperative period; however, she was otherwise cognitively intact. By utilizing the patient's home healthcare team and quickly adapting their unique communication methods during the perioperative period, we were able to provide an appropriate, safe anesthetic for this patient with LIS. CONCLUSIONS Many patients requiring an anesthetic are unable to effectively communicate due to language issues, hearing loss/mutism, neurological injury/stroke (aphasia), or developmental disabilities. The unique communication needs of this patient with LIS went beyond utilizing a translator and required the healthcare team to quickly learn a new communication method. We also discuss forms of intraoperative monitoring that can be used to differentiate consciousness from the anesthetized state in LIS patients, as well as making recommendations for future care of such patients.
为无法与麻醉团队进行轻松有效的沟通的患者提供安全的麻醉护理存在许多独特的挑战。沟通可能会受到语言的限制,可以通过翻译服务来解决,也可能会受到如中风或创伤性脑损伤等神经疾病的限制,这些问题不容易解决。在这种情况下,无法有效沟通可能会导致焦虑,并对患者-麻醉师关系产生负面影响,尤其是当更高的认知功能得以保留时。
我们报告了一例闭锁综合征(LIS)患者,该患者因常规结肠镜检查而到我们的内镜单位就诊。该患者只能通过眼球运动和眨眼来进行交流,因此限制了我们在围手术期评估其疼痛或其他需求的能力;然而,她的认知功能完好无损。通过利用患者的家庭保健团队,并在围手术期迅速采用他们独特的沟通方式,我们能够为这位患有 LIS 的患者提供适当、安全的麻醉。
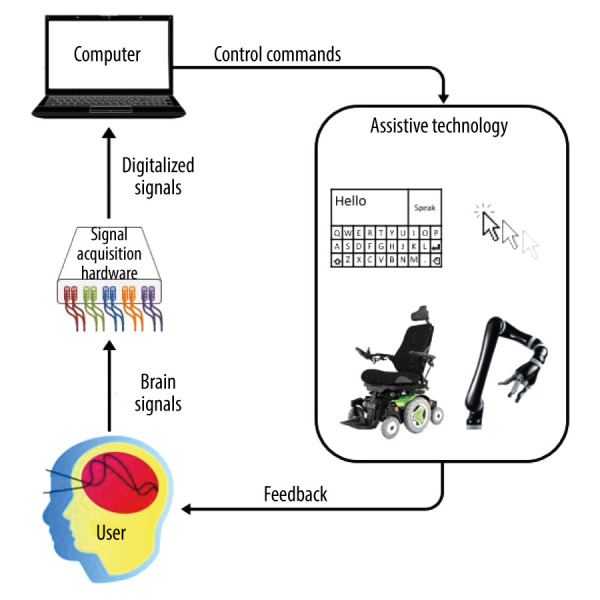
许多需要麻醉的患者由于语言问题、听力损失/缄默、神经损伤/中风(失语症)或发育障碍而无法进行有效的沟通。这位患有 LIS 的患者的独特沟通需求超出了使用翻译的范畴,需要医疗团队迅速学习一种新的沟通方式。我们还讨论了可用于区分 LIS 患者意识与麻醉状态的术中监测方式,并对今后此类患者的护理提出了建议。