Unit of Infectious Disease, Department of Medicine, Surgery and Pharmacy, University of Sassari, 07100, Sassari, Italy.
PhD School in Biomedical Science, Biomedical Science Department, University of Sassari, Sassari, Italy.
Eur J Med Res. 2024 Feb 15;29(1):123. doi: 10.1186/s40001-024-01718-6.
Several scores aimed at predicting COVID-19 progression have been proposed. As the variables vaccination and early SARS-CoV-2 treatment were systematically excluded from the prognostic scores, the present study's objective was to develop a new model adapted to the current epidemiological scenario.
We included all patients evaluated by the Infectious Disease Unit in Sassari, with SARS-CoV-2 infection and without signs of respiratory failure at the first evaluation (P/F > 300). Disease progression was defined by the prescription of supplemental oxygen. In addition, variables related to demographics, vaccines, comorbidities, symptoms, CT scans, blood tests, and therapies were collected. Multivariate logistic regression modelling was performed to determine factors associated with progression; any variable with significant univariate test or clinical relevance was selected as a candidate for multivariate analysis. Hosmer-Lemeshow (HL) goodness of fit statistic was calculated. Odds ratio values were used to derive an integer score for developing an easy-to-use progression risk score. The discrimination performance of the risk index was determined using the AUC, and the best cut-off point, according to the Youden index, sensitivity, specificity, predictive value, and likelihood ratio, was chosen.
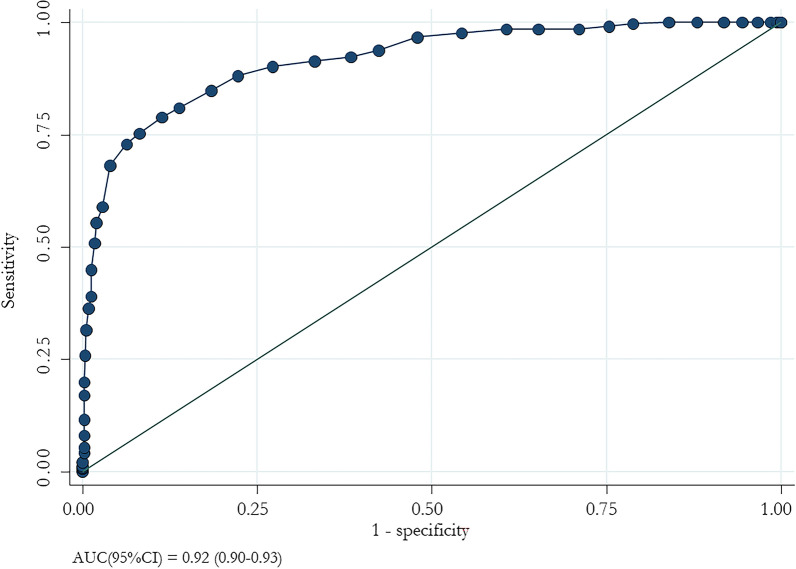
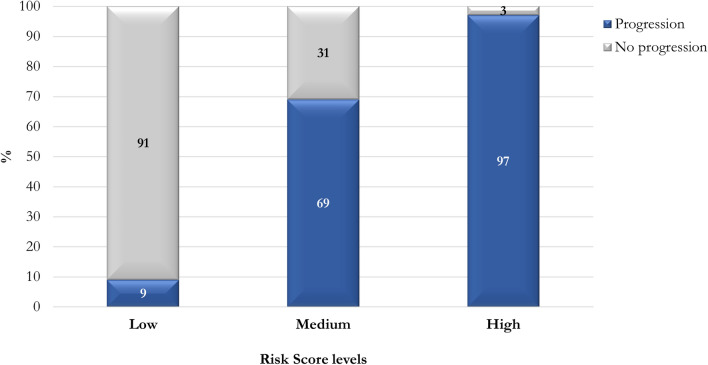
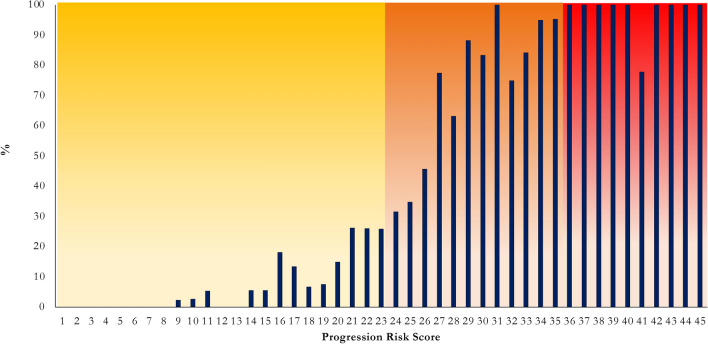
1145 patients [median (IQR) age 74 (62-83) years; 53.5% males] were enrolled; 336 (29.3%) had disease progression. Patients with a clinical progression were older and showed more comorbidities; furthermore, they were less vaccinated and exposed to preventive therapy. In the multivariate logistic regression analysis, age ≥ 60 years, COPD, dementia, haematological tumours, heart failure, exposure to no or one vaccine dose, fever, dyspnoea, GGO, consolidation, ferritin, De Ritis ≥ 1.2, LDH, and no exposure to early anti-SARS-CoV-2 treatment were associated with disease progression. The final risk score ranged from 0 to 45. The ROC curve analysis showed an AUC of 0.92 (95% CI 0.90-0.93) with a 93.7% specificity and 72.9% sensitivity. Low risk was defined when the cut-off value was less than 23. Three risk levels were identified: low (0-23 points), medium (24-35), and high (≥ 36).
The proportion of patients with progression increases with high scores: the assessment of the risk could be helpful for clinicians to plan appropriate therapeutic strategies.
已经提出了几种旨在预测 COVID-19 进展的评分。由于疫苗接种和早期 SARS-CoV-2 治疗等变量已从预后评分中系统排除,因此本研究的目的是开发一种适应当前流行病学情况的新模型。
我们纳入了在萨萨里传染病科评估的所有 SARS-CoV-2 感染患者,在首次评估时无呼吸衰竭迹象(P/F > 300)。疾病进展定义为补充氧气的处方。此外,收集了与人口统计学、疫苗接种、合并症、症状、CT 扫描、血液检查和治疗相关的变量。进行多变量逻辑回归模型以确定与进展相关的因素;任何具有显著单变量检验或临床相关性的变量均被选为多变量分析的候选变量。计算 Hosmer-Lemeshow(HL)拟合优度统计量。比值比(OR)值用于为开发易于使用的进展风险评分生成整数评分。使用 AUC 确定风险指数的判别性能,并根据约登指数、敏感性、特异性、预测值和似然比选择最佳截断值。
共纳入 1145 例患者[中位数(IQR)年龄 74(62-83)岁;53.5%为男性];336 例(29.3%)发生疾病进展。有临床进展的患者年龄较大,合并症较多;此外,他们接种疫苗较少,接受预防性治疗较少。多变量逻辑回归分析显示,年龄≥60 岁、COPD、痴呆、血液系统肿瘤、心力衰竭、接种疫苗剂量为 0 或 1 剂、发热、呼吸困难、磨玻璃影、实变、铁蛋白、De Ritis≥1.2、乳酸脱氢酶和未早期接受抗 SARS-CoV-2 治疗与疾病进展相关。最终风险评分范围为 0 至 45 分。ROC 曲线分析显示 AUC 为 0.92(95%CI 0.90-0.93),特异性为 93.7%,敏感性为 72.9%。当截断值小于 23 时,定义为低风险。确定了三个风险水平:低(0-23 分)、中(24-35 分)和高(≥36 分)。
随着评分的升高,进展患者的比例增加:评估风险有助于临床医生制定适当的治疗策略。