Han Qiao-Song, Zhou Yue, Xu Ying, Ai Kai-Liang, Song Jing-Yan, Sun Zhen-Gao
The First Clinical College, Shandong University of Traditional Chinese Medicine, Jinan, China.
The College of Traditional Chinese Medicine, Shandong University of Traditional Chinese Medicine, Jinan, Shandong, China.
Front Endocrinol (Lausanne). 2024 Feb 5;15:1340230. doi: 10.3389/fendo.2024.1340230. eCollection 2024.
Several studies have compared the effects of fixed and flexible gonadotropin releasing hormone antagonist (GnRH-ant) protocols during fertilization and embryo transfer (IVF-ET). However, which GnRH-ant initiation strategy is better remains controversial. Moreover, no studies have assessed the optimal timing of GnRH-ant initiation in women of advanced maternal age (AMA).
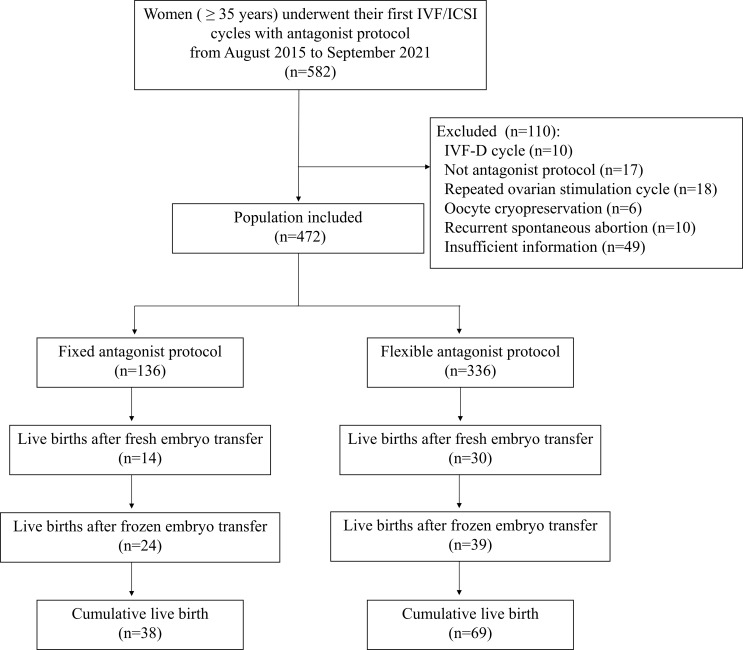
In this retrospective cohort study, a total of 472 infertile women aged ≥ 35 years old undergoing their first IVF cycle from August 2015 to September 2021 at a tertiary academic medical center were recruited, of whom 136 followed fixed GnRH-ant protocol and 336 followed flexible GnRH-ant protocol. The primary outcomes measured were the cumulative live birth rate (CLBR) per IVF cycle and the time to live birth (TTLB) from the date of oocyte retrieval. Cox proportional models were used to calculate the hazard ratio (HR) and 95% confidence interval (CI) of CLBR regarding GnRH-ant timing.
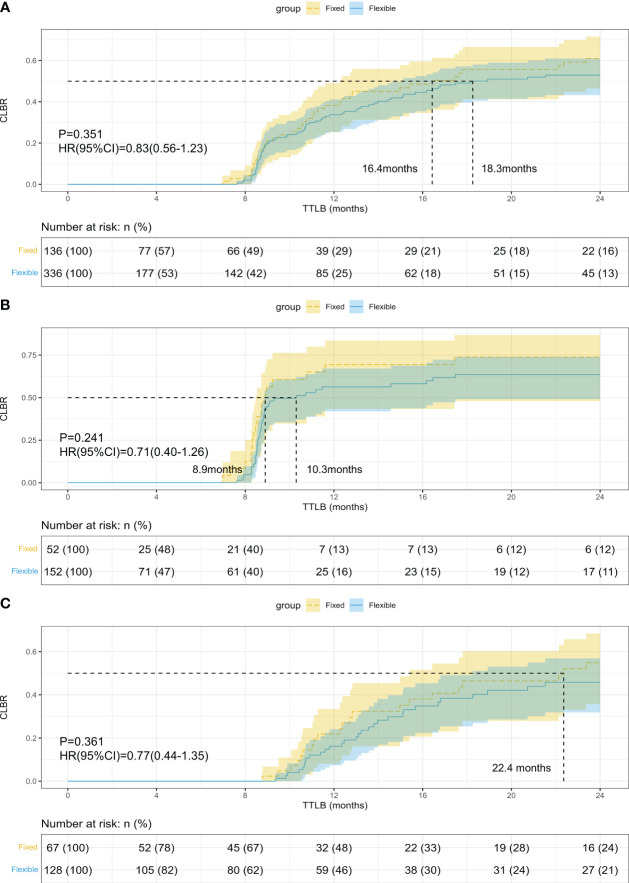
No significant difference in CLBR was found between the fixed and flexible GnRH-ant groups (27.9% vs 20.5%, p=0.105). The TTLB was also comparable between groups (10.56 vs 10.30 months, p=0.782). The Kaplan-Meier analysis for CLBR also showed comparable results between groups (P=0.351, HR=0.83; 95%CI: 0.56-1.23). After establishing a multiple Cox proportional hazard model, the fixed GnRH-ant group still had comparable CLBR with the flexible GnRH-ant group (HR=0.85; 95%CI: 0.53-1.38; P=0.518). Subgroup and sensitivity analyses also demonstrated similar results.
GnRH-ant protocols can be tailored to the needs of AMA women, and timing of GnRH-ant initiation can be adjusted flexibly.
多项研究比较了固定和灵活促性腺激素释放激素拮抗剂(GnRH-ant)方案在体外受精-胚胎移植(IVF-ET)过程中的效果。然而,哪种GnRH-ant启动策略更好仍存在争议。此外,尚无研究评估高龄产妇(AMA)中GnRH-ant启动的最佳时机。
在这项回顾性队列研究中,招募了2015年8月至2021年9月在一家三级学术医疗中心进行首次IVF周期的472名年龄≥35岁的不孕妇女,其中136名遵循固定GnRH-ant方案,336名遵循灵活GnRH-ant方案。测量的主要结局是每个IVF周期的累积活产率(CLBR)以及从取卵日期到活产的时间(TTLB)。使用Cox比例模型计算关于GnRH-ant时机的CLBR的风险比(HR)和95%置信区间(CI)。
固定和灵活GnRH-ant组之间的CLBR无显著差异(27.9%对20.5%,p = 0.105)。两组之间的TTLB也相当(10.56对10.30个月,p = 0.782)。CLBR的Kaplan-Meier分析也显示两组结果相当(P = 0.351,HR = 0.83;95%CI:0.56 - 1.23)。建立多因素Cox比例风险模型后,固定GnRH-ant组的CLBR仍与灵活GnRH-ant组相当(HR = 0.85;95%CI:0.53 - 1.38;P = 0.518)。亚组和敏感性分析也显示了相似的结果。
GnRH-ant方案可根据AMA女性的需求进行调整,GnRH-ant启动的时机可灵活调整。