Huang Ying, Lu Yao, Wang Jun, Lu Qiang, Bao Hai-Feng, Liu Lang, Dong Chun-Shan
Department of Anaesthesiology, Anhui Medical University Third Affiliated Hospital (Hefei First People's Hospital), Hefei, Anhui, People's Republic of China.
Department of Anaesthesiology, Anhui Medical University First Affiliated Hospital, Hefei, Anhui, People's Republic of China.
J Pain Res. 2024 Feb 14;17:677-685. doi: 10.2147/JPR.S445000. eCollection 2024.
The pericapsular nerve group (PENG) block provides satisfactory postoperative analgesia without hampering motor function for total hip arthroplasty (THA); however, unexpected motor block has been observed clinically. It is unknown whether this motor block is related to the dose of ropivacaine. We aimed to conduct a prospective randomized trial to test whether reducing the volume or concentration of ropivacaine was better for less motor block after PENG block.
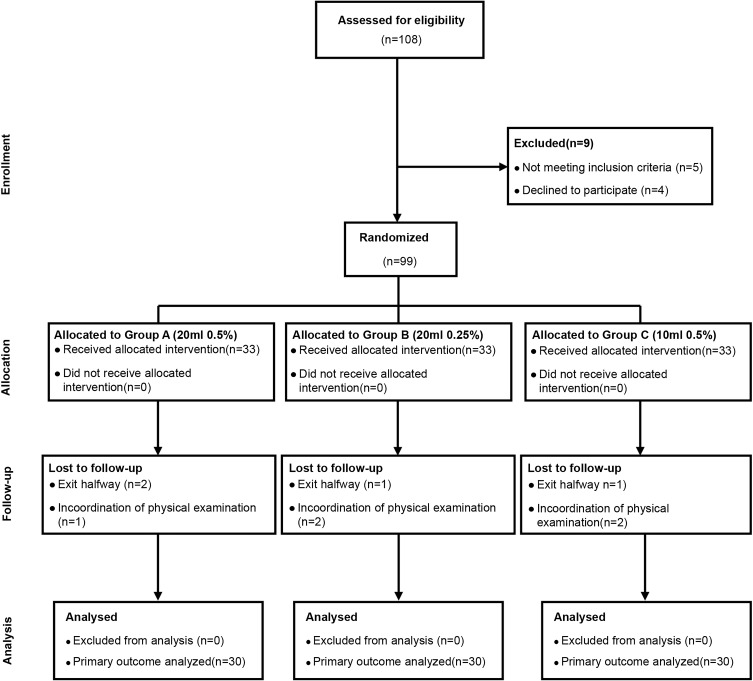
Ninety-nine patients with fracture or femoral head necrosis scheduled for THA were randomly allocated to receive 20 mL 0.5% ropivacaine (Group A), 20 mL 0.25% ropivacaine (Group B), and 10 mL 0.5% ropivacaine (Group C). The primary outcome was the incidence of postoperative quadriceps motor block at 6 hours. Secondary outcomes were the incidence of postoperative quadriceps motor block at 0, 12, 24 and 48 hours; pain scores on the numeric rating scale (NRS) at all postoperative time points (0, 6, 12, 24, and 48 hours); the time to first walk; the incidence of rescue analgesia; side effects such as dizziness, ache, nausea, and vomiting; and patient satisfaction.
Compared with Group A, Group C resulted in a lower incidence of quadriceps motor block at 0 hours, 6 hours and 12 hours postoperatively (P < 0.05), while Group B only resulted in a lower incidence of motor block at 12 hours postoperatively (P < 0.05). No intergroup differences were found in terms of postoperative pain scores, the incidence of rescue analgesia, adverse events or patient satisfaction (P > 0.05).
A higher incidence of motor blockade was observed when 20 mL of 0.5% ropivacaine was administered, which was mainly caused by the excessive volume. Therefore, we recommend performing PENG block with 10 mL 0.5% ropivacaine.
关节囊周围神经组(PENG)阻滞可为全髋关节置换术(THA)提供满意的术后镇痛,且不影响运动功能;然而,临床上已观察到意外的运动阻滞。尚不清楚这种运动阻滞是否与罗哌卡因的剂量有关。我们旨在进行一项前瞻性随机试验,以测试减少罗哌卡因的体积或浓度是否更有利于减少PENG阻滞后的运动阻滞。
99例计划行THA的骨折或股骨头坏死患者被随机分配接受20 mL 0.5%罗哌卡因(A组)、20 mL 0.25%罗哌卡因(B组)和10 mL 0.5%罗哌卡因(C组)。主要结局是术后6小时股四头肌运动阻滞的发生率。次要结局包括术后0、12、24和48小时股四头肌运动阻滞的发生率;所有术后时间点(0、6、12、24和48小时)的数字评分量表(NRS)疼痛评分;首次行走时间;补救镇痛的发生率;头晕、疼痛、恶心和呕吐等副作用;以及患者满意度。
与A组相比,C组术后0小时、6小时和12小时股四头肌运动阻滞的发生率较低(P<0.05),而B组仅在术后12小时运动阻滞的发生率较低(P<0.05)。术后疼痛评分、补救镇痛的发生率、不良事件或患者满意度方面未发现组间差异(P>0.05)。
给予20 mL 0.5%罗哌卡因时观察到较高的运动阻滞发生率,这主要是由过量的体积所致。因此,我们建议使用10 mL 0.5%罗哌卡因进行PENG阻滞。