Pfizer, Inc., Pharm Sci and PGS Statistics, Groton, Connecticut, United States of America.
Department of Applied Statistics and Research Methods, University of Northern Colorado, Greeley, Colorado, United States of America.
PLoS One. 2024 Feb 26;19(2):e0272684. doi: 10.1371/journal.pone.0272684. eCollection 2024.
Stunting is common among children in many low and middle income countries, particularly in rural and urban slum settings. Few studies have described child stunting transitions and the associated factors in urban slum settlements. We describe transitions between stunting states and associated factors among children living in Nairobi slum settlements.
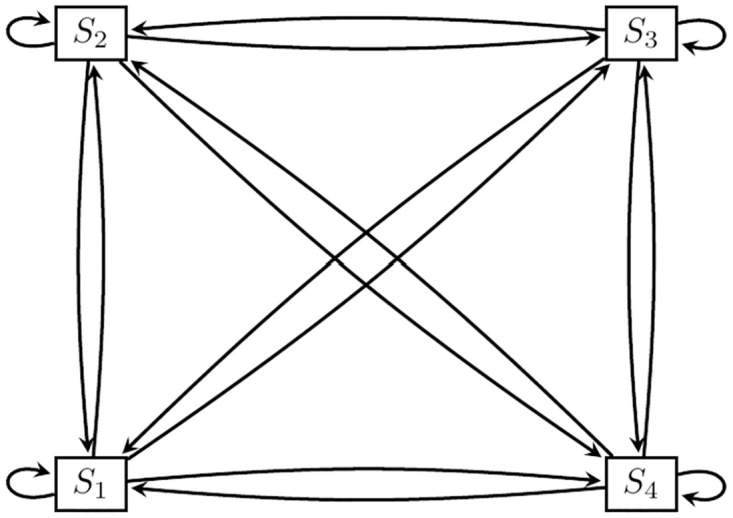
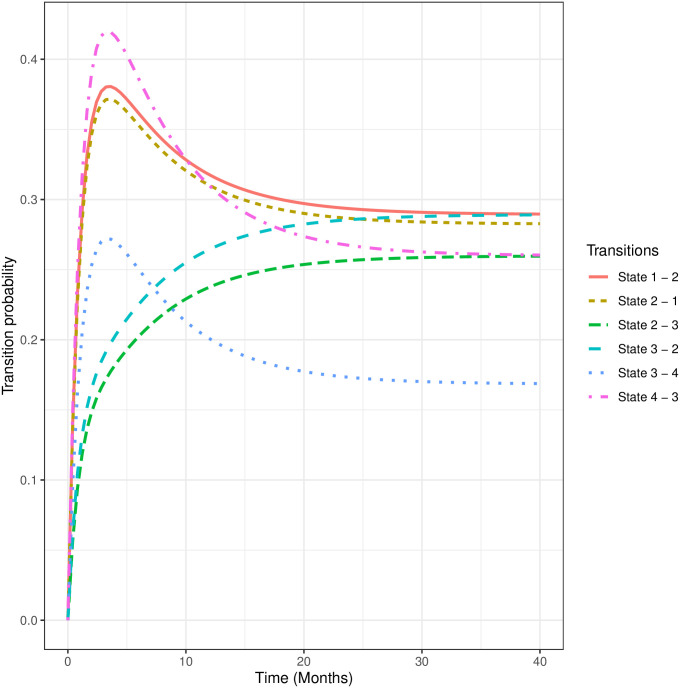
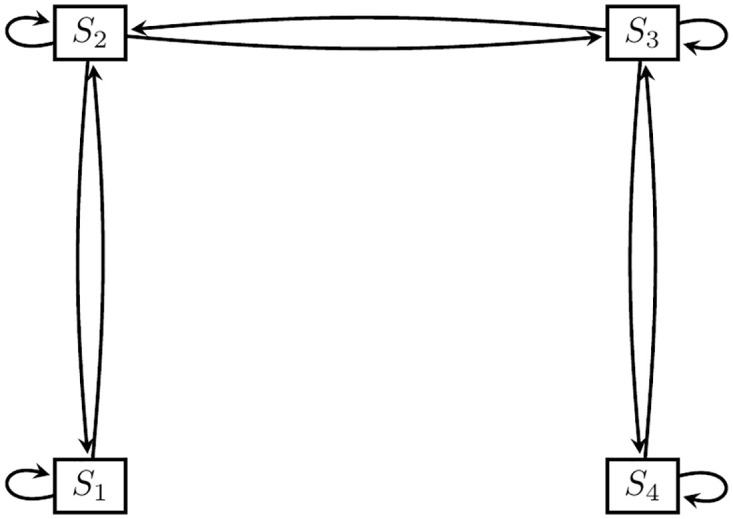
This study used data collected between 2010 and 2014 from the Nairobi Urban and Demographic Surveillance System (NUHDSS) and a vaccination study nested within the surveillance system. A subset of 692 children aged 0 to 3 years, with complete anthropometric data, and household socio-demographic data was used for the analysis. Height-for-age Z-scores (HAZ) was used to define stunting: normal (HAZ ≥ 1), marginally stunted (-2 ≤ HAZ < -1), moderately stunted (-3 ≤ HAZ < -2), and severely stunted (HAZ < -3). Transitions from one stunting level to another and in the reverse direction were computed. The associations between explanatory factors and the transitions between four child stunting states were modeled using a continuous-time multi-state model.
We observed that 48%, 39%, 41%, and 52% of children remained in the normal, marginally stunted, moderately stunted, and severely stunted states, respectively. About 29% transitioned from normal to marginally stunted state, 15% to the moderately stunted state, and 8% to the severely stunted state. Also, 8%, 12%, and 29% back transitioned from severely stunted, moderately stunted, and marginally stunted states, to the normal state, respectively. The shared common factors associated with all transitions to a more severe state include: male gender, ethnicity (only for mild and severe transition states), child's age, and household food insecurity. In Korogocho, children whose parents were married and those whose mothers had attained primary or post-primary education were associated with a transition from a mild state into a moderately stunted state. Children who were breastfed exclusively were less likely to transition from moderate to severe stunting state.
These findings reveal a high burden of stunting and transitions in urban slums. Context-specific interventions targeting the groups of children identified by the socio-demographic factors are needed. Improving food security and exclusive breastfeeding could potentially reduce stunting in the slums.
在许多低收入和中等收入国家,儿童发育迟缓很常见,尤其是在农村和城市贫民窟地区。很少有研究描述过城市贫民窟中儿童发育迟缓的转变及其相关因素。我们描述了内罗毕贫民窟中儿童发育迟缓状态的转变及其相关因素。
本研究使用了 2010 年至 2014 年期间在内罗毕城市和人口监测系统(NUHDSS)以及监测系统内嵌套的疫苗接种研究中收集的数据。使用了一组 692 名 0 至 3 岁的儿童,他们具有完整的人体测量数据和家庭社会人口学数据,用于分析。身高年龄 Z 分数(HAZ)用于定义发育迟缓:正常(HAZ≥1),边缘发育迟缓(-2≤HAZ<-1),中度发育迟缓(-3≤HAZ<-2)和严重发育迟缓(HAZ<-3)。计算了从一个发育迟缓水平到另一个水平的转变以及相反方向的转变。使用连续时间多状态模型对解释因素与四个儿童发育迟缓状态之间的转变之间的关联进行建模。
我们观察到,分别有 48%、39%、41%和 52%的儿童分别保持在正常、边缘发育迟缓、中度发育迟缓以及严重发育迟缓状态。大约 29%的儿童从正常状态转变为边缘发育迟缓状态,15%的儿童转变为中度发育迟缓状态,8%的儿童转变为严重发育迟缓状态。此外,8%、12%和 29%的儿童分别从严重发育迟缓、中度发育迟缓以及边缘发育迟缓状态向后过渡到正常状态。与所有向更严重状态转变相关的共同因素包括:性别(仅与轻度和重度转变状态相关)、民族(仅与轻度和重度转变状态相关)、儿童年龄以及家庭粮食不安全。在科罗戈乔,父母已婚以及母亲接受过小学或中学后教育的儿童与从轻度状态向中度发育迟缓状态的转变有关。接受纯母乳喂养的儿童不太可能从中度转变为严重发育迟缓状态。
这些发现揭示了城市贫民窟中发育迟缓及其转变的高负担。需要针对社会人口因素确定的儿童群体制定具体的干预措施。改善粮食安全和纯母乳喂养可能会降低贫民窟的发育迟缓率。