Translational Research Center, University Hospital of Psychiatry and Psychotherapy, University of Bern, Bern, Switzerland.
Graduate School for Health Sciences, University of Bern, Bern, Switzerland.
JAMA Psychiatry. 2024 Jun 1;81(6):563-571. doi: 10.1001/jamapsychiatry.2024.0026.
Psychomotor slowing is a frequent symptom of psychosis, impairing gross and fine motor behavior. It is associated with poor outcomes and functioning, and no treatment is available.
To investigate whether 15 sessions of inhibitory repetitive transcranial magnetic stimulation (rTMS) may reduce psychomotor slowing.
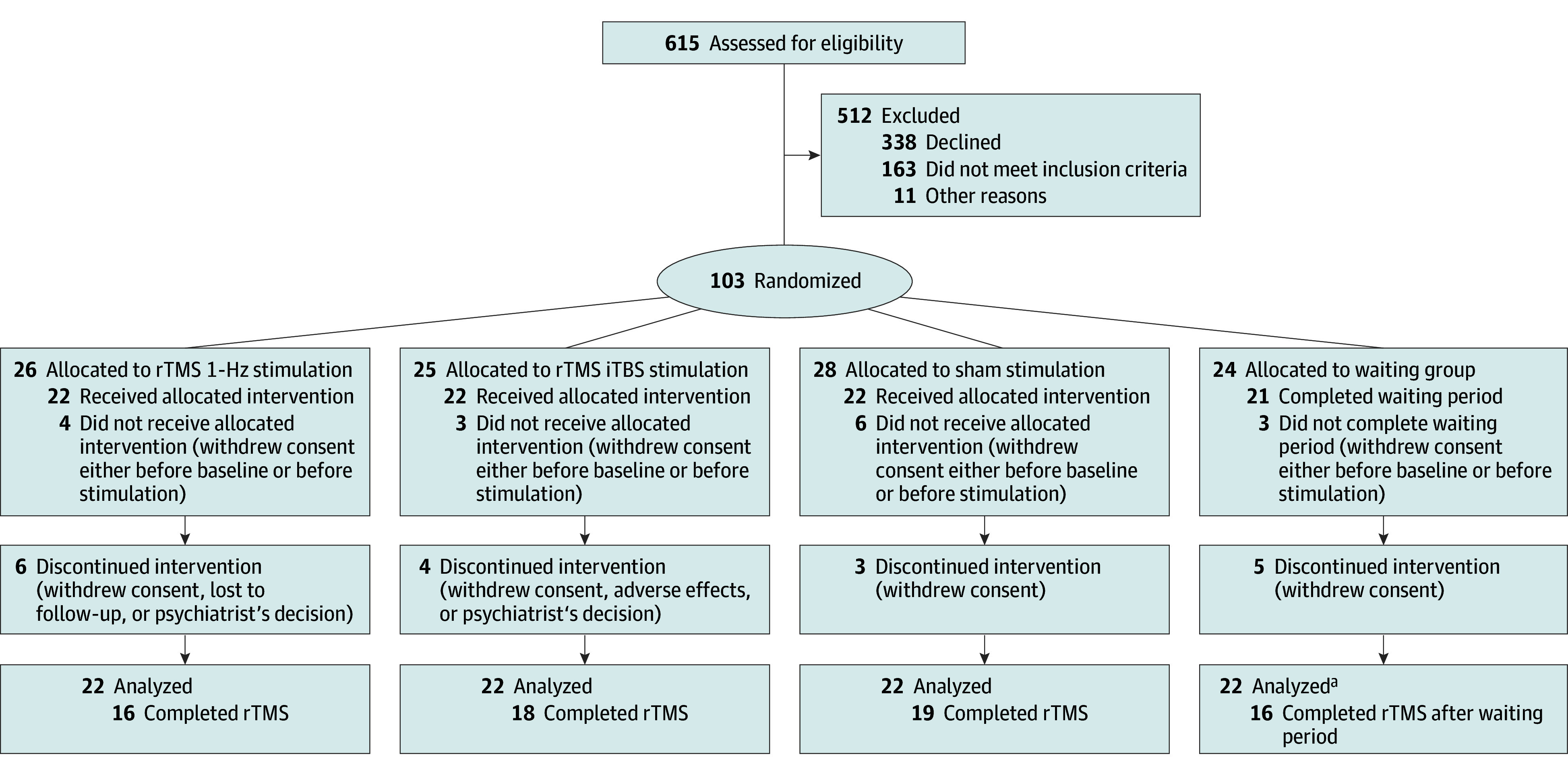
DESIGN, SETTING, AND PARTICIPANTS: This was a 4-arm, double-blind, randomized, sham-controlled trial at a university hospital in Switzerland. Enrollment took place from March 2019 to August 2022. Adults aged 18 to 60 years with schizophrenia spectrum disorders and severe psychomotor slowing were eligible. All patients continued existing medications, including antipsychotics and benzodiazepines. Those with substance misuse (other than nicotine), conditions associated with impaired or aberrant movement, convulsions, history of hearing problems, other conditions typically excluded from magnetic resonance imaging or TMS, any TMS treatment in the past 3 months, or those who were pregnant or breastfeeding were excluded. Of 615 patients screened for eligibility, 103 were randomized and 88 received at least 1 session of rTMS: 22 were assigned to 1-Hz rTMS, 22 to iTBS, 22 to sham, and 22 to the waiting group. Follow-up was conducted at 6 weeks and 24 weeks following the week 3 assessments including clinical, functional, and motor measures.
Fifteen sessions of rTMS in 3 weeks over the supplementary motor area: 1-Hz rTMS, iTBS, sham, or no treatment (waiting). After 3 weeks, the waiting group received 15 sessions of 1-Hz rTMS over the supplementary motor area.
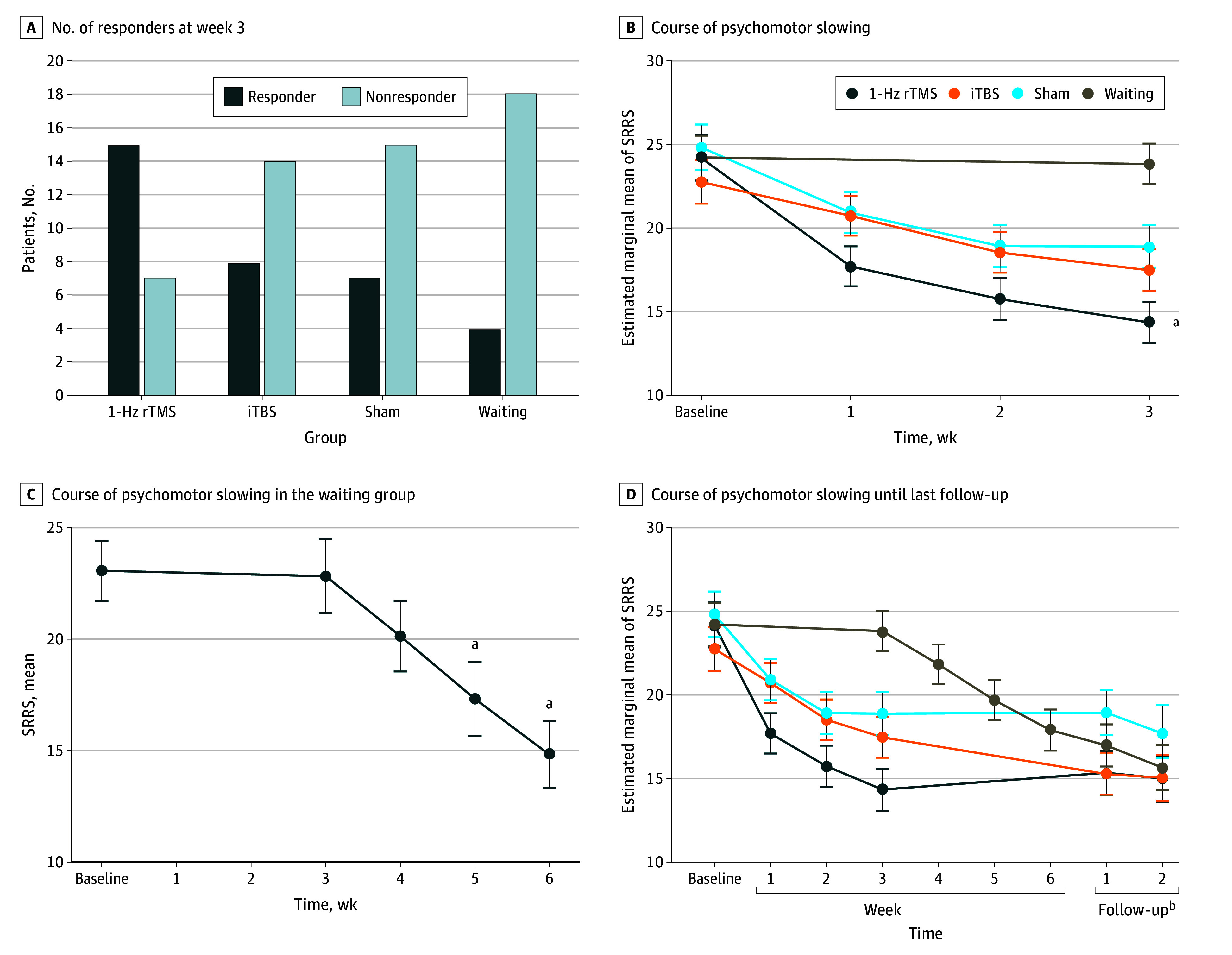
The main outcome was the proportion of responders at week 3 in the Salpêtrière Retardation Rating Scale (SRRS) defined as a 30% or greater reduction from baseline (last-observation-carried-forward). The SRRS has 15 items and a maximum total score of 60.
Of the 88 participants analyzed, 45 were men and 43 were women. The mean (SD) age was 36.3 (12.4) years and the mean (SD) SRRS score was 24.0 (5.9). A total of 69 participants completed the study. At week 3, response rates differed between groups: 15 of 22 (68%) in the 1-Hz rTMS group, 8 of 22 (36%) in the iTBS group, 7 of 22 (32%) in the sham group, and 4 of 22 (18%) in the waiting group (χ23 = 12.1; P = .007). The 1-Hz rTMS group had more responders than sham (odds ratio [OR], 0.13; 95% CI, 0.02-0.65; P = .03), iTBS (OR, 0.12; 95% CI, 0.02-0.61; P = .02), and waiting (OR, 0.04; 95% CI, 0.01-0.22; P = .003). In the waiting group, 10 of 16 participants (63%) responded after receiving 15 sessions of 1-Hz rTMS. No serious adverse events occurred.
In this study, inhibitory add-on rTMS safely alleviated psychomotor slowing in psychosis compared with iTBS, sham, and no treatment. The treatment was also effective with delayed onset. Future studies need to explore the neural changes associated with supplementary motor area rTMS in psychosis.
ClinicalTrials.gov Identifier: NCT03921450.
重要性:精神运动迟缓是精神病的常见症状,会损害粗大运动和精细运动行为。它与较差的结果和功能有关,目前尚无治疗方法。
目的:研究 15 次抑制性重复经颅磁刺激(rTMS)是否可以减轻精神运动迟缓。
设计、地点和参与者:这是一项在瑞士一所大学医院进行的 4 臂、双盲、随机、假对照试验。招募时间为 2019 年 3 月至 2022 年 8 月。符合条件的患者为年龄在 18 至 60 岁之间的精神分裂症谱系障碍且精神运动迟缓严重的成年人。所有患者均继续使用现有药物,包括抗精神病药和苯二氮䓬类药物。有物质滥用(除尼古丁外)、与运动受损或异常相关的疾病、癫痫发作、听力问题史、磁共振成像或 TMS 通常排除的其他疾病、过去 3 个月内接受过任何 TMS 治疗或怀孕或哺乳的患者被排除在外。在筛选出的 615 名符合条件的患者中,有 103 名被随机分配,88 名接受了至少 1 次 rTMS 治疗:22 名接受 1-Hz rTMS 治疗,22 名接受 iTBS 治疗,22 名接受假治疗,22 名接受等待治疗。在第 3 周评估后 6 周和 24 周进行随访,包括临床、功能和运动测量。
干预措施:3 周内通过重复经颅磁刺激治疗补充运动区 15 次:1-Hz rTMS、iTBS、假刺激或不治疗(等待)。3 周后,等待组接受补充运动区 1-Hz rTMS 治疗 15 次。
主要结果和措施:主要结果是 Salpêtrière 延迟评分量表(SRRS)在第 3 周的应答比例,定义为与基线相比减少 30%或更多(最后观察到的进展)。SRRS 有 15 个项目,总分最高为 60 分。
结果:在分析的 88 名参与者中,45 名是男性,43 名是女性。平均(SD)年龄为 36.3(12.4)岁,平均(SD)SRRS 评分为 24.0(5.9)。共有 69 名参与者完成了研究。在第 3 周,各组的应答率不同:1-Hz rTMS 组 22 名中有 15 名(68%),iTBS 组 22 名中有 8 名(36%),假刺激组 22 名中有 7 名(32%),等待组 22 名中有 4 名(18%)(χ23=12.1;P=0.007)。1-Hz rTMS 组的应答者多于假刺激组(比值比[OR],0.13;95%CI,0.02-0.65;P=0.03)、iTBS 组(OR,0.12;95%CI,0.02-0.61;P=0.02)和等待组(OR,0.04;95%CI,0.01-0.22;P=0.003)。在等待组中,16 名参与者中有 10 名(63%)在接受 15 次 1-Hz rTMS 治疗后出现反应。没有发生严重不良事件。
结论和相关性:在这项研究中,与 iTBS、假刺激和不治疗相比,抑制性附加 rTMS 可安全缓解精神病中的精神运动迟缓。该治疗方法还具有延迟起效的效果。未来的研究需要探索精神分裂症补充运动区 rTMS 相关的神经变化。
试验注册:ClinicalTrials.gov 标识符:NCT03921450。