Department of Anesthesiology, University Medical Centre of the Johannes Gutenberg-University Mainz, Mainz, Germany.
Institute of Medical Biostatistics, Epidemiology and Informatics, University Medical Centre of the Johannes Gutenberg-University Mainz, Mainz, Germany.
PLoS One. 2024 Mar 1;19(3):e0299071. doi: 10.1371/journal.pone.0299071. eCollection 2024.
While awake tracheal intubation (ATI) is regarded as the gold standard for difficult airway management according to current guidelines, there seems to be a reluctance in its application. This retrospective cohort study, conducted at a German tertiary hospital over a 2-year period, aimed to demonstrate that integrating awake tracheal intubation using flexible bronchoscopy (ATI:FB) into routine airway management makes it a successful and safe approach.
In 2019 and 2020, records from the data acquisition system (DAQ) and archived anesthesia records were screened to evaluate the specifics of ATI:FB procedures, focusing on overall success and safety. Analysis included complications, time required for ATI:FB, and potential influencing factors such as patient characteristics, indication, medical/operative specialty, sedation technique, route and experience of anesthesiologist. Logistic regression assessed the impact of various variables on occurrence of complications and linear regression, with log(time) as the dependent variable, evaluated median time required to perform ATI:FB.
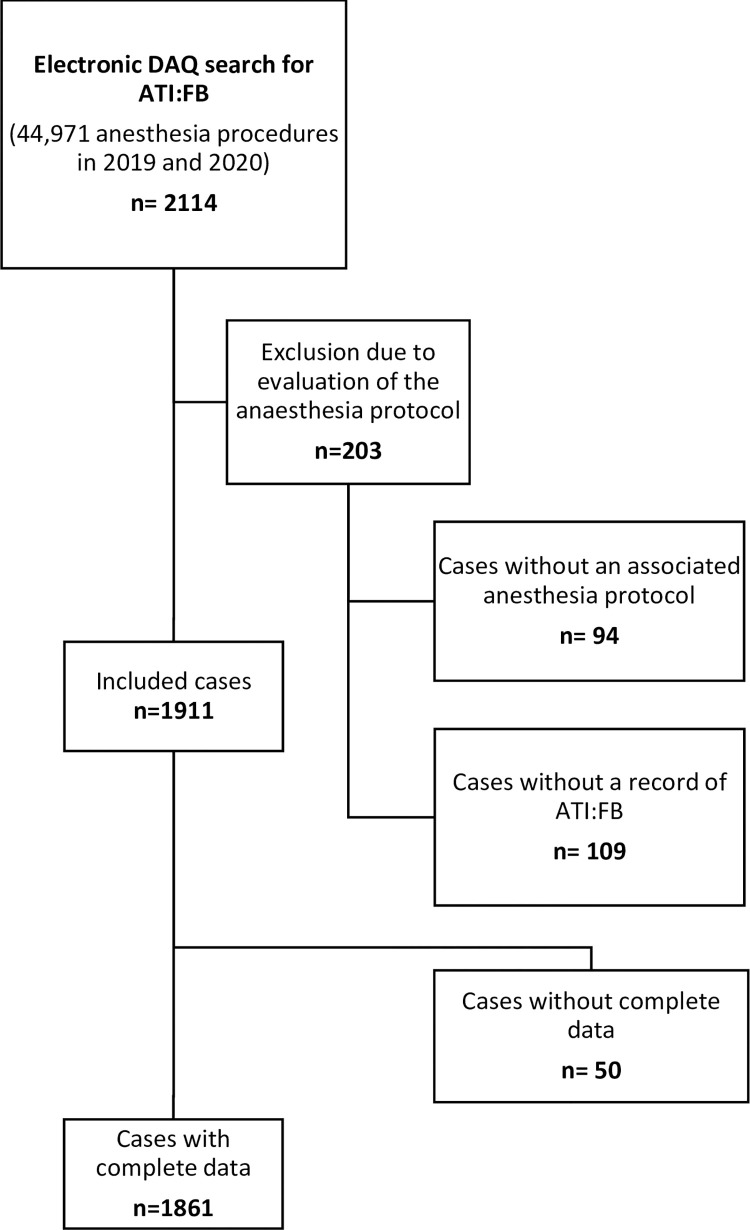
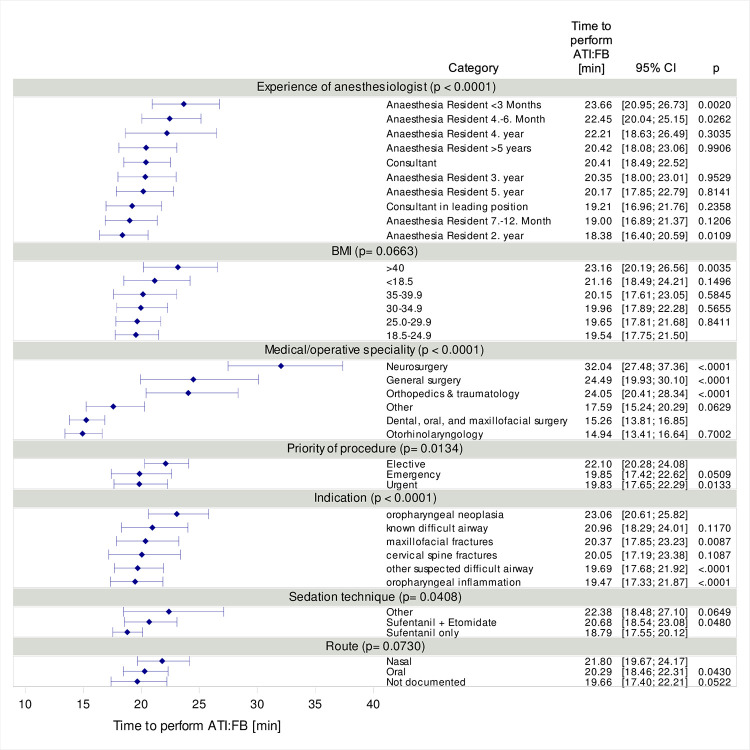
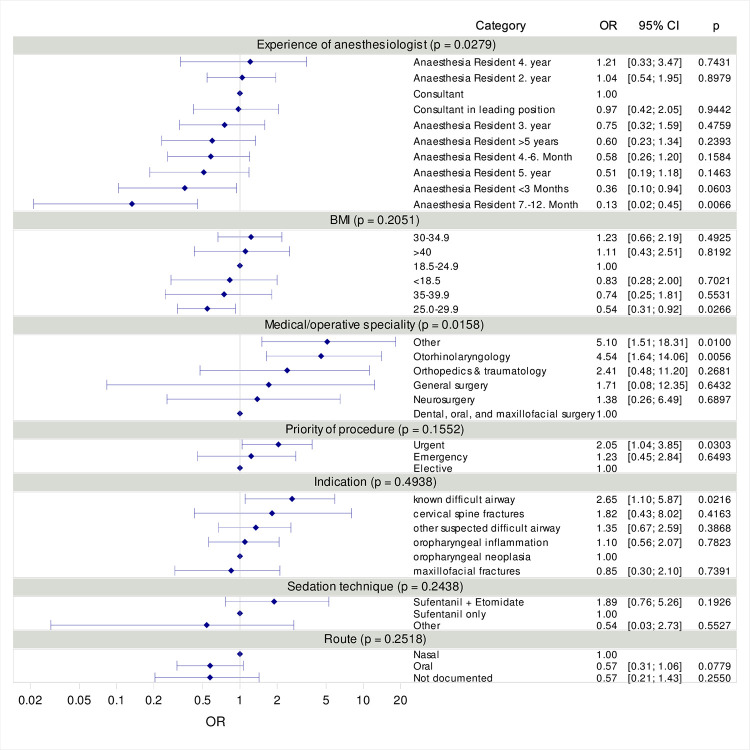
ATI:FB constituted 4.3 % (n = 1,911) of all airway management procedures, predominantly observed in dental, oral, and maxillofacial surgery (46.5 %) and otorhinolaryngology (38.4 %). The success rate for ATI:FB was notably high at 99.6 %, with only 5.4 % of cases experiencing complications, including technical issues, agitation, and visibility obstruction due to mucous secretion. Complication risk was influenced by the medical specialty and the experience of the anesthesiologist. A strong effect was observed in otorhinolaryngology (OR = 4.54, 95 % CI [1.64; 14.06]). The median time required for ATI:FB was 16 minutes (IQR: 11 to 23), with factors such as indication (p < 0.0001), experience of anesthesiologist (p < 0.0001), sedation technique (p = 0.0408), priority of the procedure (p = 0.0134), and medical/operative specialty (p < 0.0001) affecting the duration. The median time required for ATI:FB differed significantly based on the experience of the anesthesiologist (p < 0.0001).
ATI:FB proves successful and safe, with low complications and manageable procedural time. Experience of the anesthesiologist is a modifiable factor enhancing safety, emphasizing the need for ATI:FB integration into routine airway management.
根据目前的指南,清醒气管插管(ATI)在清醒状态下进行被认为是困难气道管理的金标准,但在实际应用中似乎存在抵触情绪。本研究在德国一家三级医院进行,回顾性分析了两年间的病例,旨在证明将使用柔性支气管镜的清醒气管插管(ATI:FB)整合到常规气道管理中是一种成功且安全的方法。
2019 年和 2020 年,通过数据采集系统(DAQ)和存档的麻醉记录筛选病例,评估 ATI:FB 程序的具体情况,重点关注整体成功率和安全性。分析包括并发症、ATI:FB 所需时间以及患者特征、适应证、医学/手术专业、镇静技术、麻醉医生入路和经验等潜在影响因素。使用逻辑回归评估各种变量对并发症发生的影响,使用线性回归,以 log(time)为因变量,评估 ATI:FB 所需的中位时间。
ATI:FB 占所有气道管理程序的 4.3%(n=1911),主要见于牙科、口腔和颌面外科(46.5%)和耳鼻喉科(38.4%)。ATI:FB 的成功率非常高,达到 99.6%,仅有 5.4%的病例出现并发症,包括技术问题、躁动和因粘液分泌导致的可视度障碍。并发症风险受医学专业和麻醉医生经验的影响。耳鼻喉科的影响作用明显(OR=4.54,95%CI[1.64;14.06])。ATI:FB 所需的中位时间为 16 分钟(IQR:11 至 23),适应证(p<0.0001)、麻醉医生经验(p<0.0001)、镇静技术(p=0.0408)、操作优先级(p=0.0134)和医学/手术专业(p<0.0001)等因素均影响操作时间。ATI:FB 所需的中位时间因麻醉医生经验而异(p<0.0001)。
ATI:FB 安全且有效,并发症发生率低,操作时间可管理。麻醉医生的经验是一个可改变的因素,可以提高安全性,强调将 ATI:FB 整合到常规气道管理中的必要性。