Bostel Tilman, Nikolaidou Eirini, Wollschläger Daniel, Mayer Arnulf, Kaufmann Justus, Hopprich Anne, Rühle Alexander, Grosu Anca-Ligia, Debus Jürgen, Fottner Christian, Moehler Markus, Grimminger Peter, Schmidberger Heinz, Nicolay Nils Henrik
Department of Radiation Oncology, University Medical Center Mainz, Langenbeckstraße 1, 55131, Mainz, Germany.
German Cancer Consortium (DKTK) Partner Site Mainz, German Cancer Research Center (Dkfz), Heidelberg, Germany.
Radiat Oncol. 2024 Mar 4;19(1):28. doi: 10.1186/s13014-024-02414-9.
To assess the tolerability and oncological results of chemoradiation in elderly patients with locally advanced adenocarcinoma of the esophagus or gastroesophageal junction.
This multi-center retrospective analysis included 86 elderly patients (≥ 65 years) with esophageal or gastroesophageal junction adenocarcinoma (median age 73 years; range 65-92 years) treated with definitive or neoadjuvant (chemo)radiotherapy. The treatment was performed at 3 large comprehensive cancer centers in Germany from 2006 to 2020. Locoregional control (LRC), progression-free survival (PFS), distant metastasis-free survival (DMFS), overall survival (OS), and treatment-associated toxicities according to CTCAE criteria v5.0 were analyzed, and parameters potentially relevant to patient outcomes were evaluated.
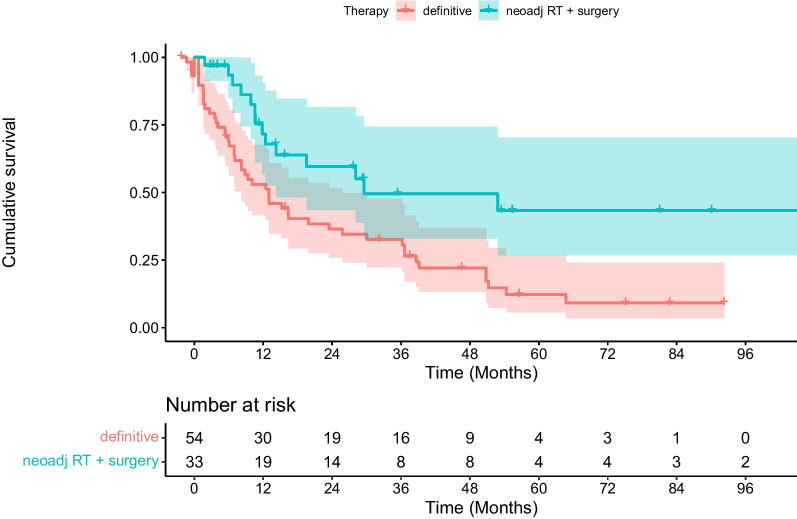
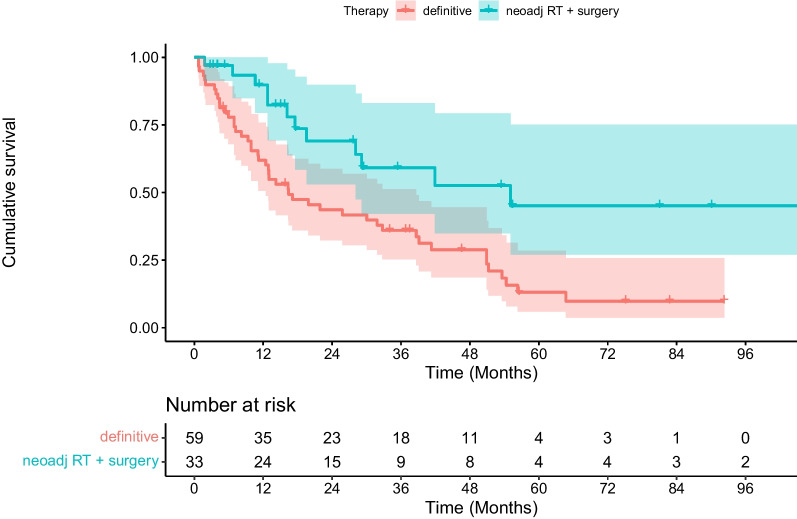
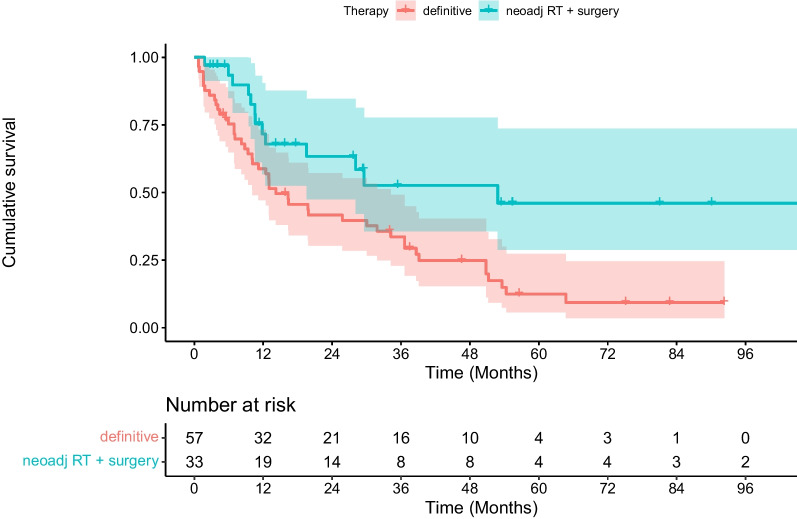
Thirty-three patients (38%) were treated with neoadjuvant chemoradiation followed by surgery, while the remaining patients received definitive (chemo)radiation. The delivery of radiotherapy without dose reduction was possible in 80 patients (93%). In 66 patients (77%), concomitant chemotherapy was initially prescribed; however, during the course of therapy, 48% of patients (n = 32) required chemotherapy de-escalation due to treatment-related toxicities and comorbidities. Twenty-nine patients (34%) experienced higher-grade acute toxicities and 14 patients (16%) higher-grade late toxicities. The 2-year LRC, DMFS, PFS, and OS amounted to 72%, 49%, 46%, and 52%, respectively. In multivariate analysis, neoadjuvant chemoradiation followed by surgery was shown to be associated with significantly better PFS (p = 0.006), DMFS (p = 0.006), and OS (p = 0.004) compared with all non-surgical treatments (pooled definitive radiotherapy and chemoradiation). No such advantage was seen over definitive chemoradiation. The majority of patients with neoadjuvant therapy received standard chemoradiotherapy without dose reduction (n = 24/33, 73%). In contrast, concurrent chemotherapy was only possible in 62% of patients undergoing definitive radiotherapy (n = 33/53), and most of these patients required dose-reduction or modification of chemotherapy (n = 23/33, 70%).
In our analysis, omission of chemotherapy or adjustment of chemotherapy dose during definitive radiotherapy was necessary for the overwhelming majority of elderly esophageal cancer patients not eligible for surgery, and hence resulted in reduced PFS and OS. Therefore, optimization of non-surgical approaches and the identification of potential predictive factors for safe administration of concurrent chemotherapy in elderly patients with (gastro)esophageal adenocarcinoma is required.
评估老年局部晚期食管腺癌或食管胃交界腺癌患者接受放化疗的耐受性及肿瘤学疗效。
这项多中心回顾性分析纳入了86例老年患者(≥65岁),他们患有食管或食管胃交界腺癌(中位年龄73岁;范围65 - 92岁),接受了根治性或新辅助(化疗)放疗。治疗于2006年至2020年在德国3家大型综合癌症中心进行。根据CTCAE v5.0标准分析局部区域控制(LRC)、无进展生存期(PFS)、无远处转移生存期(DMFS)、总生存期(OS)以及治疗相关毒性,并评估可能与患者预后相关的参数。
33例患者(38%)接受了新辅助放化疗后手术,其余患者接受了根治性(化疗)放疗。80例患者(93%)能够在不降低剂量的情况下进行放疗。66例患者(77%)最初处方了同步化疗;然而,在治疗过程中,48%的患者(n = 32)由于治疗相关毒性和合并症需要降低化疗强度。29例患者(34%)出现了高级别急性毒性,14例患者(16%)出现了高级别晚期毒性。2年的LRC、DMFS、PFS和OS分别为72%、49%、46%和52%。在多变量分析中,与所有非手术治疗(汇总的根治性放疗和放化疗)相比,新辅助放化疗后手术显示出与显著更好的PFS(p = 0.006)、DMFS(p = 0.006)和OS(p = 0.004)相关。与根治性放化疗相比未见此类优势。大多数接受新辅助治疗的患者接受了不降低剂量的标准放化疗(n = 24/33,73%)。相比之下,在接受根治性放疗的患者中,只有62%的患者(n = 33/53)能够进行同步化疗,并且这些患者中的大多数需要降低化疗剂量或调整化疗方案(n = 23/33,70%)。
在我们的分析中,对于绝大多数不符合手术条件的老年食管癌患者,在根治性放疗期间省略化疗或调整化疗剂量是必要的,因此导致PFS和OS降低。因此,需要优化非手术方法,并确定老年食管(胃)腺癌患者安全进行同步化疗的潜在预测因素。