Hochberger Jürgen, Loss Martin, Kruse Elena
Klinikum Friedrichshain, Abteilung für Gastroenterologie, Interdisziplinäres Darmkrebszentrum, Vivantes Netzwerk für Gesundheit GmbH, Berlin, Deutschland.
Lehrkrankenhaus Vivantes Friedrichshain, Gastroenterologie, Charité Universitätsmedizin Berlin, Berlin, Deutschland.
Zentralbl Chir. 2024 Feb;149(1):46-55. doi: 10.1055/a-2256-6724. Epub 2024 Mar 5.
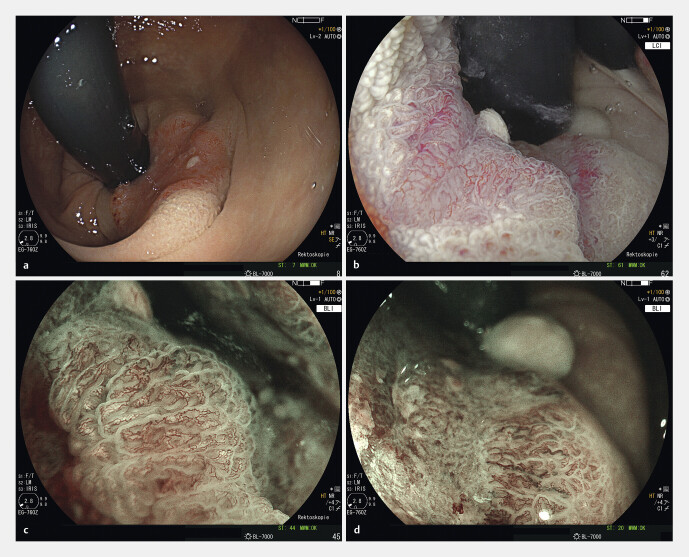
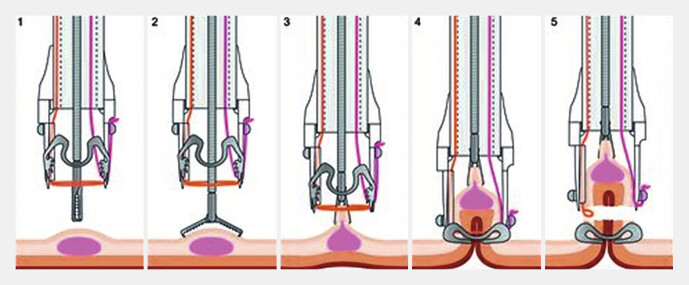
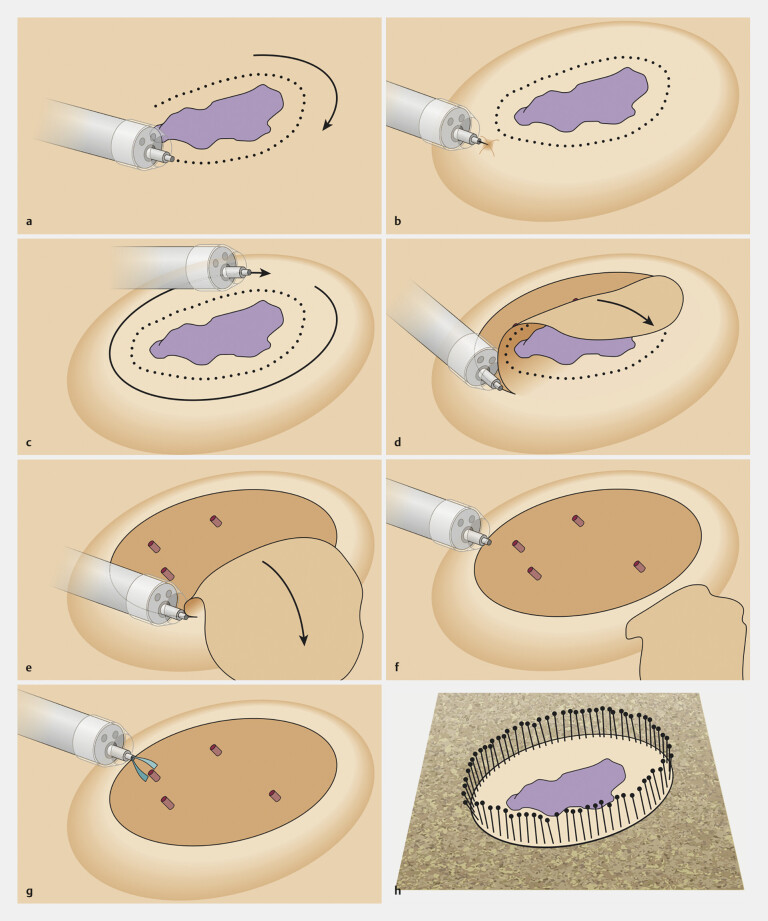
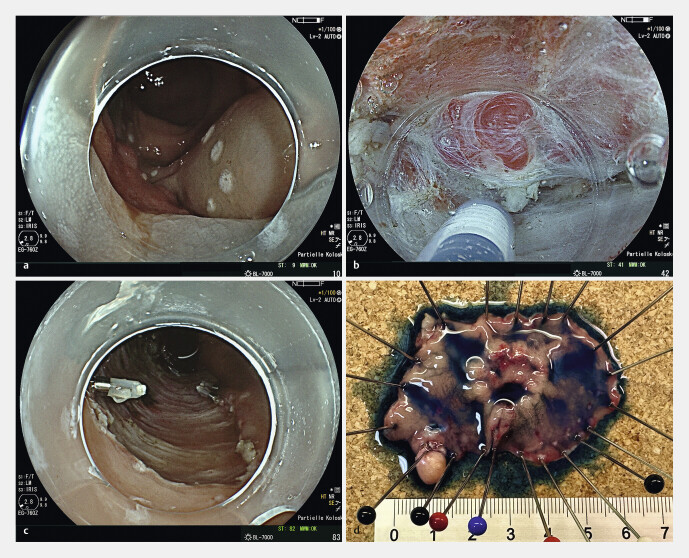
Today, endoscopy plays a decisive role not only in the detection of colorectal adenomas and carcinomas, but also in the treatment of precancerous lesions, in particular flat adenomas and early carcinomas. In recent years, endoscopic submucosal dissection (ESD) has become increasingly important alongside classic polypectomy and mucosal resection after saline injection using a snare (EMR). Using ESD the lesion is marked, injected submucosally using viscous substances and the mucosa incised and tunneled with a transparent cap and a fine diathermy knife. Particularly in the case of widespread and high-risk lesions ESD enables a quasi-surgical "en bloc" resection almost regardless of size, with a histological R0 resection rate of far over 90% in specialized centers. ESD enables an excellent histopathological evaluation and has a low recurrence risk of 1-3%. Endoscopic full-thickness resection using a dedicated device (FTRD system) represents another addition to the armamentarium. It can be used for circumscribed submucosal, suspicious or scarred changes up to 2 cm in the middle and upper rectum. Endoscopic intermuscular dissection (EID) enables histopathological analysis of the complete submucosa beyond the mucosa and upper submucosal layer by including the circular inner muscle layer within the resection specimen. It reduces basal R1 situations and offers a new perspective for T1 carcinomas through curative, organ-preserving endoscopic therapy, especially in the case of deep submucosal infiltration alone, without other risk factors for metastases. Indications, the procedure itself and significance of the various techniques for premalignant and early malignant lesions in the rectum are presented.
如今,内镜检查不仅在结直肠腺瘤和癌的检测中发挥着决定性作用,而且在癌前病变,特别是扁平腺瘤和早期癌的治疗中也起着关键作用。近年来,内镜黏膜下剥离术(ESD)与经典的息肉切除术以及使用圈套器进行盐水注射后的黏膜切除术(EMR)相比,变得越来越重要。使用ESD时,需对病变进行标记,通过注射粘性物质使其黏膜下隆起,然后使用透明帽和精细的电刀切开并剥离黏膜。特别是对于广泛且高危的病变,ESD几乎可以实现不分大小的准手术“整块”切除,在专业中心其组织学R0切除率远超过90%。ESD能够进行出色的组织病理学评估,复发风险低至1%-3%。使用专用设备的内镜全层切除术(FTRD系统)是内镜治疗手段的又一补充。它可用于直肠中上部直径达2厘米的局限性黏膜下可疑或瘢痕性病变。内镜肌层间剥离术(EID)通过在切除标本中包含环形内肌层,能够对黏膜及黏膜上层以外的完整黏膜下层进行组织病理学分析。它减少了切缘R1情况,为T1期癌提供了一种新的治疗视角,即通过内镜下根治性保器官治疗,特别是在仅存在深层黏膜下浸润且无其他转移危险因素的情况下。本文介绍了直肠癌前病变和早期恶性病变的各种技术的适应证、操作过程及其意义。