Han Yafan, Shao Mingliang, Yang Hang, Sun Huaxin, Sang Wanyue, Wang Lu, Wang Liang, Yang Suxia, Jian Yi, Tang Baopeng, Li Yaodong
Cardiac Pacing and Electrophysiology Department, The First Affiliated Hospital of Xinjiang Medical University, Urumqi, 830054, China.
Xinjiang Key Laboratory of Cardiac Electrophysiology and Cardiac Remodeling, The First Affiliated Hospital of Xinjiang Medical University, Urumqi, 830054, China.
Sci Rep. 2024 Mar 11;14(1):5926. doi: 10.1038/s41598-024-56651-9.
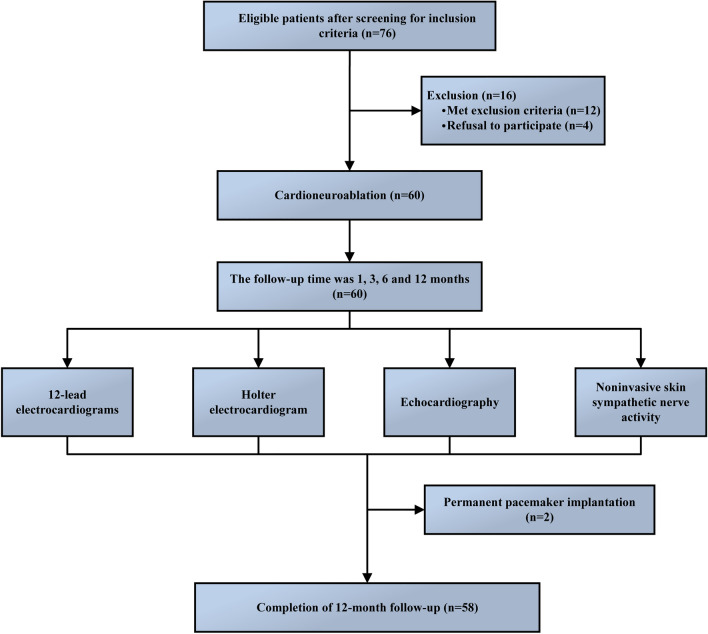
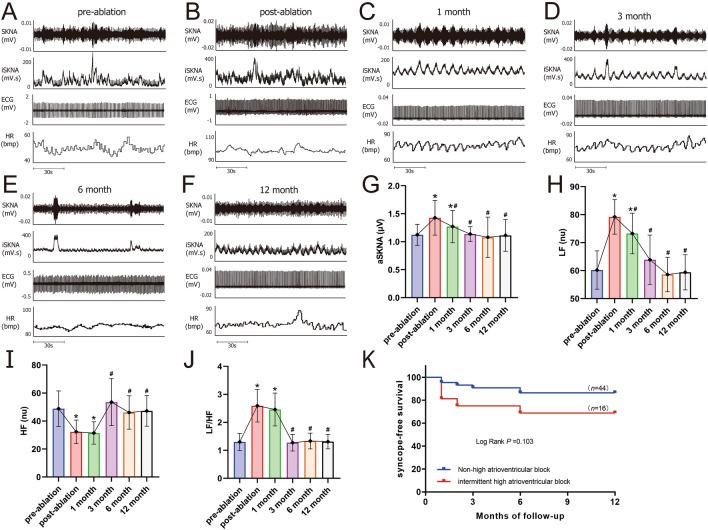
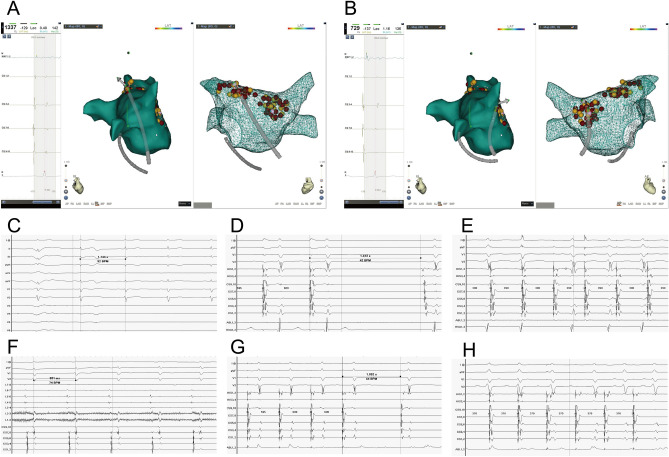
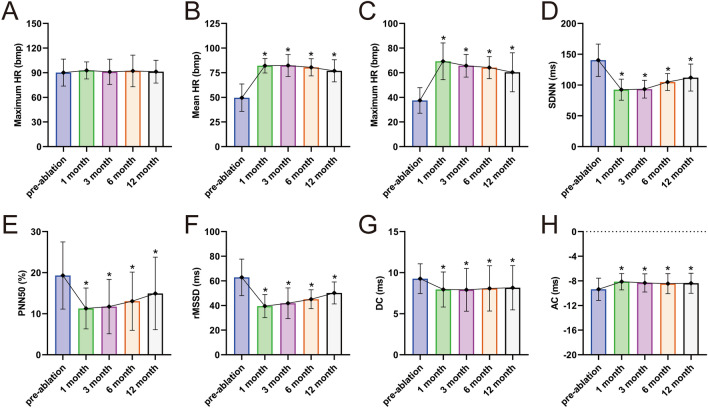
Cardioneuroablation (CNA) is currently considered as a promising treatment option for patients with symptomatic bradycardia caused by vagotonia. This study aims to further investigate its safety and efficacy in patients suffering from vagal bradycardia. A total of 60 patients with vagal bradycardia who underwent CNA in the First Affiliated Hospital of Xinjiang Medical University from November 2019 to June 2022. Preoperative atropine tests revealed abnormal vagal tone elevation in all patients. First, the electroanatomic structures of the left atrium was mapped out by using the Carto 3 system, according to the protocol of purely anatomy-guided and local fractionated intracardiac electrogram-guided CNA methods. The upper limit of ablation power of superior left ganglion (SLGP) and right anterior ganglion (RAGP) was not more than 45W with an ablation index of 450.Postoperative transesophageal cardiac electrophysiological examination was performed 1 to 3 months after surgery. The atropine test was conducted when appropriate. Twelve-lead electrocardiogram, Holter electrocardiogram, and skin sympathetic nerve activity were reviewed at 1, 3, 6 and 12 months after operation. Adverse events such as pacemaker implantation and other complications were also recorded to analyze the safety and efficacy of CNA in the treatment of vagus bradycardia. Sixty patients were enrolled in the study (38 males, mean age 36.67 ± 9.44, ranging from 18 to 50 years old). None of the patients had a vascular injury, thromboembolism, pericardial effusion, or other surgical complications. The mean heart rate, minimum heart rate, low frequency, low/high frequency, acceleration capacity of rate, and skin sympathetic nerve activity increased significantly after CNA. Conversely, SDNN, PNN50, rMSSD, high frequency, and deceleration capacity of rate values decreased after CNA (all P < 0.05). At 3 months after ablation, the average heart rate, maximum heart rate, and acceleration capacity of heart rate remained higher than those before ablation, and the deceleration capacity of heart rate remained lower than those before ablation and the above results continued to follow up for 12 months after ablation (all P < 0.05). There was no significant difference in other indicators compared with those before ablation (all P > 0.05). The remaining 81.67% (49/60) of the patients had good clinical results, with no episodes of arrhythmia during follow-up. CNA may be a safe and effective treatment for vagal-induced bradycardia, subject to confirmation by larger multicenter trials.
心脏神经消融术(CNA)目前被认为是治疗迷走神经张力过高引起的症状性心动过缓患者的一种有前景的治疗选择。本研究旨在进一步探讨其在迷走神经性心动过缓患者中的安全性和有效性。2019年11月至2022年6月期间,共有60例迷走神经性心动过缓患者在新疆医科大学第一附属医院接受了CNA治疗。术前阿托品试验显示所有患者迷走神经张力均异常升高。首先,根据纯解剖引导和局部碎裂心内电图引导的CNA方法的方案,使用Carto 3系统绘制左心房的电解剖结构。左上神经节(SLGP)和右前神经节(RAGP)的消融功率上限不超过45W,消融指数为450。术后1至3个月进行经食管心脏电生理检查。在适当的时候进行阿托品试验。术后1、3、6和12个月复查12导联心电图、动态心电图和皮肤交感神经活动。还记录了起搏器植入等不良事件和其他并发症,以分析CNA治疗迷走神经性心动过缓的安全性和有效性。60例患者纳入研究(男性38例,平均年龄36.67±9.44岁,年龄范围18至50岁)。所有患者均未发生血管损伤、血栓栓塞、心包积液或其他手术并发症。CNA术后平均心率、最低心率、低频、低频/高频、心率加速能力和皮肤交感神经活动均显著增加。相反,CNA术后SDNN、PNN50、rMSSD、高频和心率减速能力值下降(所有P<0.05)。消融术后3个月,平均心率、最大心率和心率加速能力仍高于消融前,心率减速能力仍低于消融前,上述结果在消融后持续随访12个月(所有P<0.05)。与消融前相比,其他指标无显著差异(所有P>0.05)。其余81.67%(49/60)的患者临床效果良好,随访期间无心律失常发作。CNA可能是治疗迷走神经源性心动过缓的一种安全有效的方法,但有待更大规模的多中心试验证实。