Shiozawa Aki, Mancuso Shayna, Young Christopher, Friderici Jennifer, Tran Summer, Trenz Helen M
Medical Affairs US, Astellas Pharma, Inc., 1 Astellas Way, Northbrook, IL, 60062, USA.
Optum, Eden Prairie, MN, USA.
Adv Ther. 2024 May;41(5):1885-1895. doi: 10.1007/s12325-024-02821-0. Epub 2024 Mar 11.
The study objective was to estimate all-cause healthcare resource utilization (HCRU) and medical and pharmacy costs for women with treated versus untreated vasomotor symptoms (VMS) due to menopause.
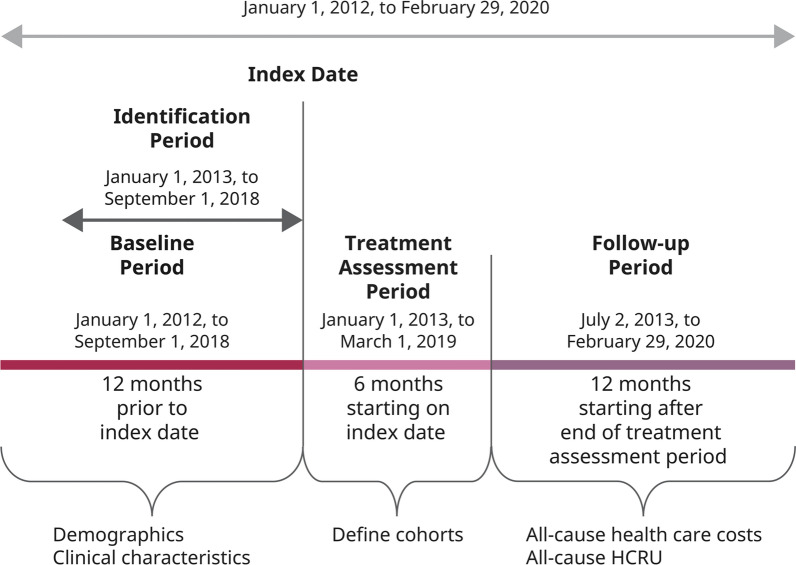
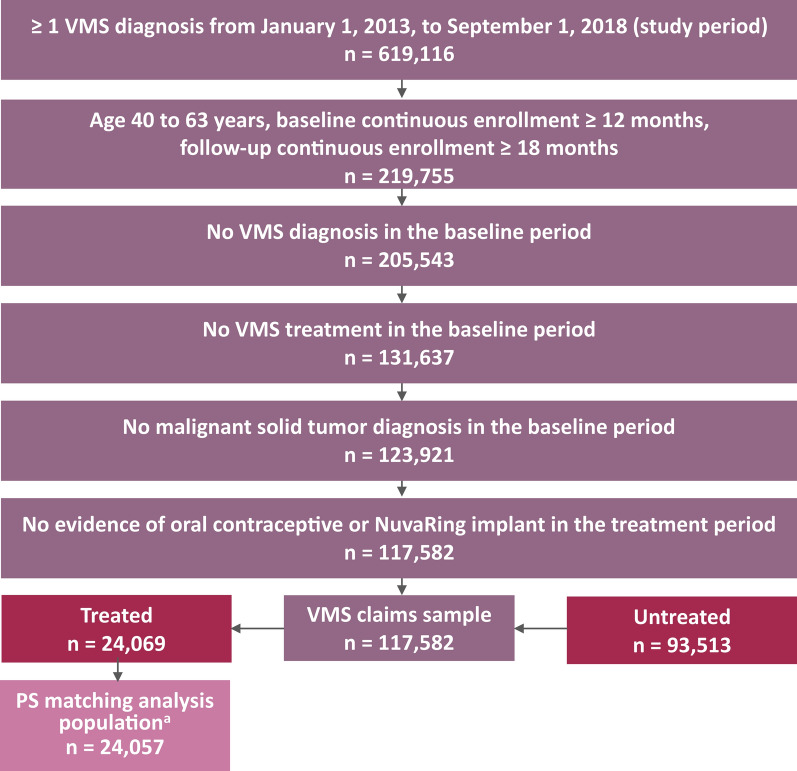
A retrospective study was conducted using US claims data from Optum Research Database (study period: January 1, 2012-February 29, 2020). Women aged 40-63 years with a VMS diagnosis claim and ≥ 12 and ≥ 18 months of continuous enrollment during baseline and follow-up periods, respectively, were included. Women treated for VMS were propensity score matched 1:1 to untreated controls with VMS. Standardized differences (SDIFF) ≥ 10% were considered meaningful. A generalized linear model (gamma distribution, log link, robust standard errors) estimated the total cost of care ratio. Subgroup analyses of on- and off-label treatment costs were conducted.
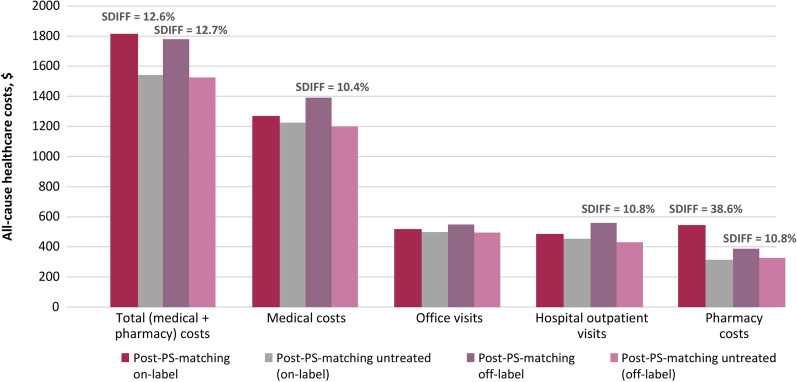
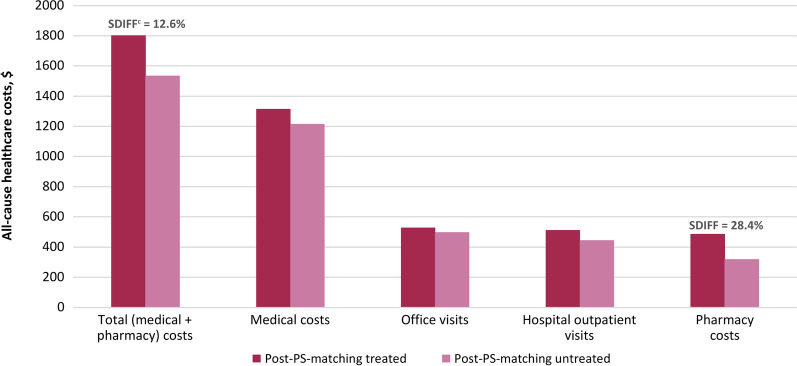
Of 117,582 women diagnosed with VMS, 20.5% initiated VMS treatment and 79.5% had no treatment. Treated women (n = 24,057) were matched to untreated VMS controls. There were no differences in HCRU at follow-up (SDIFF < 10%). Pharmacy ($487 vs $320, SDIFF 28.4%) and total ($1803 vs $1536, SDIFF 12.6%) costs were higher in the treated cohort. Total costs were 7% higher in the treated cohort (total cost ratio 1.07, 95% CI 1.05-1.10, P < 0.001). The on-label treatment pharmacy costs ($546 versus $315, SDIFF 38.6%) were higher in the treated cohort. Off-label treatment had higher medical costs ($1393 versus $1201, SDIFF 10.4%).
Most women with VMS due to menopause were not treated within 6 months following diagnosis. While both on- and off-label treatment increased the total cost of care compared with untreated controls, those increases were modest in magnitude and should not impede treatment for women who report symptom improvement as a result of treatment.
本研究的目的是估计因更年期出现血管舒缩症状(VMS)且接受治疗与未接受治疗的女性的全因医疗资源利用(HCRU)以及医疗和药房费用。
使用来自Optum研究数据库的美国索赔数据进行了一项回顾性研究(研究期间:2012年1月1日至2020年2月29日)。纳入年龄在40 - 63岁之间、有VMS诊断索赔且在基线期和随访期分别连续参保≥12个月和≥18个月的女性。接受VMS治疗的女性按倾向得分1:1与未接受治疗的VMS对照匹配。标准化差异(SDIFF)≥10%被认为有意义。采用广义线性模型(伽马分布、对数链接、稳健标准误)估计护理总成本比。进行了标签内和标签外治疗成本的亚组分析。
在117,582名被诊断为VMS的女性中,20.5%开始接受VMS治疗,79.5%未接受治疗。接受治疗的女性(n = 24,057)与未接受治疗的VMS对照匹配。随访时HCRU无差异(SDIFF < 10%)。接受治疗队列的药房费用(487美元对320美元,SDIFF 28.4%)和总费用(1803美元对1536美元,SDIFF 12.6%)更高。接受治疗队列的总费用高7%(总成本比1.07,95% CI 1.05 - 1.10,P < 0.001)。接受治疗队列的标签内治疗药房费用(546美元对315美元,SDIFF 38.6%)更高。标签外治疗的医疗费用更高(1393美元对1201美元,SDIFF 10.4%)。
大多数因更年期出现VMS的女性在诊断后6个月内未接受治疗。虽然与未接受治疗的对照相比,标签内和标签外治疗均增加了护理总成本,但这些增加幅度不大,不应妨碍因治疗而症状改善的女性接受治疗。