Yoshizaki Moegi, Matsuo Yasuko, Yasuda Satoshi, Doi Shunsuke, Sakata Takeshi, Nagai Minako, Nakamura Kota, Kohara Yuichiro, Toyoda Shohei, Tanaka Toshihiro, Sho Masayuki
Department of Surgery, Nara Medical University, 840 Shijo-Cho, Kashihara, Nara, 634-8522, Japan.
Department of Radiology, Nara Medical University, 840 Shijo-Cho, Kashihara, Nara, 634-8522, Japan.
Surg Case Rep. 2024 Mar 15;10(1):60. doi: 10.1186/s40792-024-01845-6.
Ehlers-Danlos syndrome (EDS) is a genetic disorder that causes fragility of the systemic connective tissues. Of the 13 subtypes, vascular EDS (vEDS) is associated with abnormalities in collagen production, resulting in arterial rupture and intestinal perforation. Herein, we report the case of a man with confirmed vEDS who survived a ruptured dissected splenic artery aneurysm triggered by perforation of the sigmoid colon.
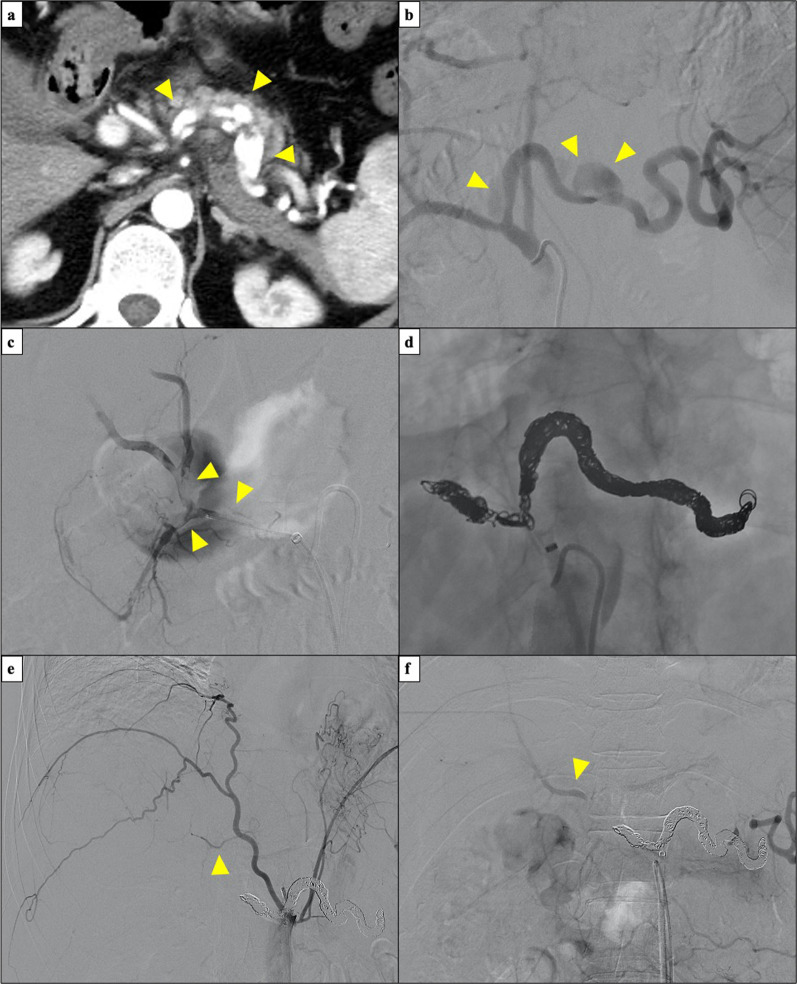
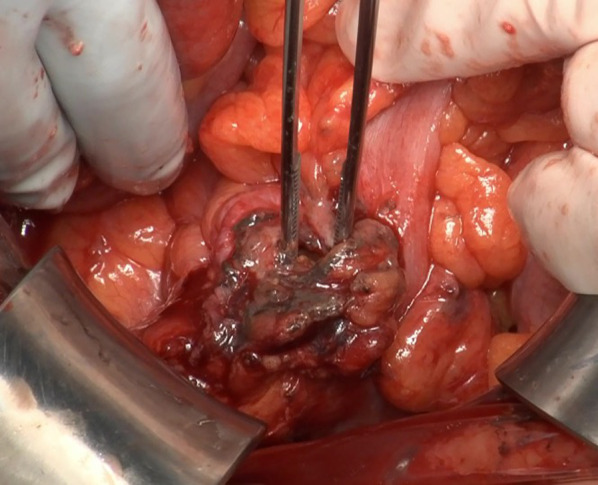
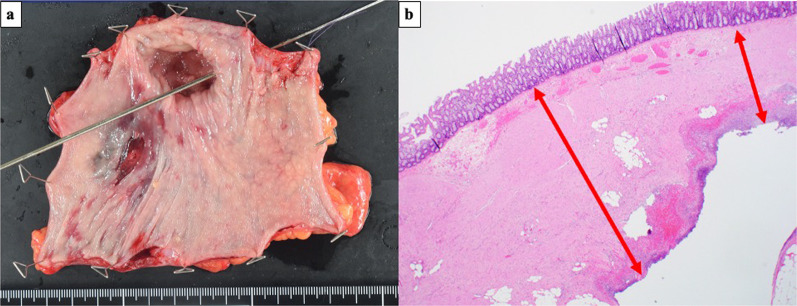
A 48-year-old man presented to our hospital with sudden severe lower abdominal pain. The patient was genetically diagnosed with vEDS at the age of 43 years. Abdominal computed tomography (CT) showed fluid and free air surrounding the sigmoid colon. These findings suggested sigmoid colon perforation, and emergency surgery was needed. Hartmann's procedure was performed. The resected specimen showed a 2-cm-sized depression around the perforation. Histopathological findings showed an abscess and exudate in the serosa of the perforation and thinning of the intrinsic muscular layer in the depressed area. The patient was doing well postoperatively; however, on the ninth postoperative day, sudden upper abdominal pain developed. CT revealed an intra-abdominal hemorrhage due to rupture of a dissecting splenic artery aneurysm. The aneurysm was not observed on preoperative CT and was distant from the surgical site. Urgent transcatheter arterial embolization was performed. Although embolization of the splenic artery was attempted during the procedure, the arterial dissection spread to the common hepatic artery. Moreover, the proper hepatic and gastroduodenal arteries were poorly visualized, probably due to vasospasm. Although complications associated with extensive embolization were a concern, embolization of the splenic and common hepatic arteries was necessary to save the patient's life. After embolization, angiography showed that the left hepatic blood flow was maintained from the inferior phrenic artery, and the right hepatic inflow was maintained from the superior mesenteric artery via the peribiliary vascular plexus in the hilar area. The patient recovered well and was discharged on the 19th postoperative day.
vEDS can cause arterial rupture after intestinal surgery. Therefore, careful post-operative management is necessary. Moreover, cooperation with interventional radiologists is important for prompt treatment of vascular complications.
埃勒斯-当洛综合征(EDS)是一种遗传性疾病,可导致全身结缔组织脆弱。在13种亚型中,血管型EDS(vEDS)与胶原蛋白生成异常有关,可导致动脉破裂和肠穿孔。在此,我们报告一例确诊为vEDS的男性患者,他在乙状结肠穿孔引发的脾动脉夹层动脉瘤破裂后存活下来。
一名48岁男性因突发严重下腹痛入院。该患者在43岁时经基因诊断为vEDS。腹部计算机断层扫描(CT)显示乙状结肠周围有液体和游离气体。这些发现提示乙状结肠穿孔,需要进行急诊手术。实施了哈特曼手术。切除的标本显示穿孔周围有一个2厘米大小的凹陷。组织病理学检查结果显示穿孔处浆膜有脓肿和渗出物,凹陷区域固有肌层变薄。患者术后恢复良好;然而,术后第9天突然出现上腹痛。CT显示脾动脉夹层动脉瘤破裂导致腹腔内出血。术前CT未发现该动脉瘤,且其与手术部位距离较远。进行了紧急经导管动脉栓塞术。尽管在手术过程中尝试对脾动脉进行栓塞,但动脉夹层蔓延至肝总动脉。此外,可能由于血管痉挛,肝固有动脉和胃十二指肠动脉显示不清。尽管广泛栓塞相关的并发症令人担忧,但为挽救患者生命,仍有必要对脾动脉和肝总动脉进行栓塞。栓塞后,血管造影显示左肝血流由膈下动脉维持,右肝血流由肠系膜上动脉通过肝门区的胆管周围血管丛维持。患者恢复良好,术后第19天出院。
vEDS可导致肠道手术后动脉破裂。因此,术后需仔细管理。此外,与介入放射科医生合作对于及时治疗血管并发症很重要。