Department of Medicine, University of Washington, Seattle, WA; Clinical Research Division, Fred Hutchinson Cancer Center, Seattle, WA.
Department of Medicine, University of Washington, Seattle, WA; Clinical Research Division, Fred Hutchinson Cancer Center, Seattle, WA.
Clin Lymphoma Myeloma Leuk. 2024 Jul;24(7):446-454.e3. doi: 10.1016/j.clml.2024.02.013. Epub 2024 Feb 23.
Patients with multiple myeloma (MM) may be on therapy for years, which can lead to financial toxicity (FinTox) or time toxicity (TimeTox). The prevalence, predictors, and quality of life (QOL) impacts of FinTox and TimeTox during different phases of MM treatment have not been characterized.
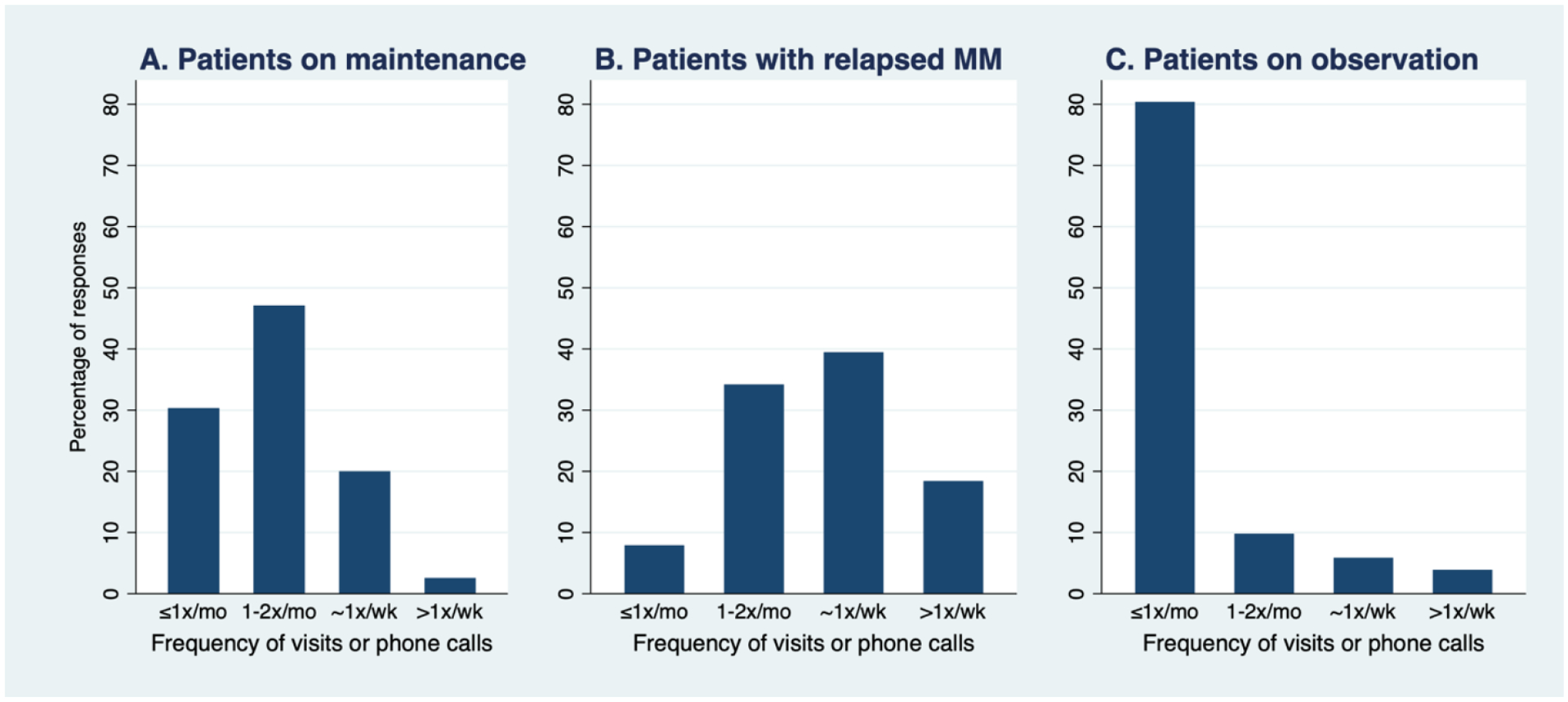
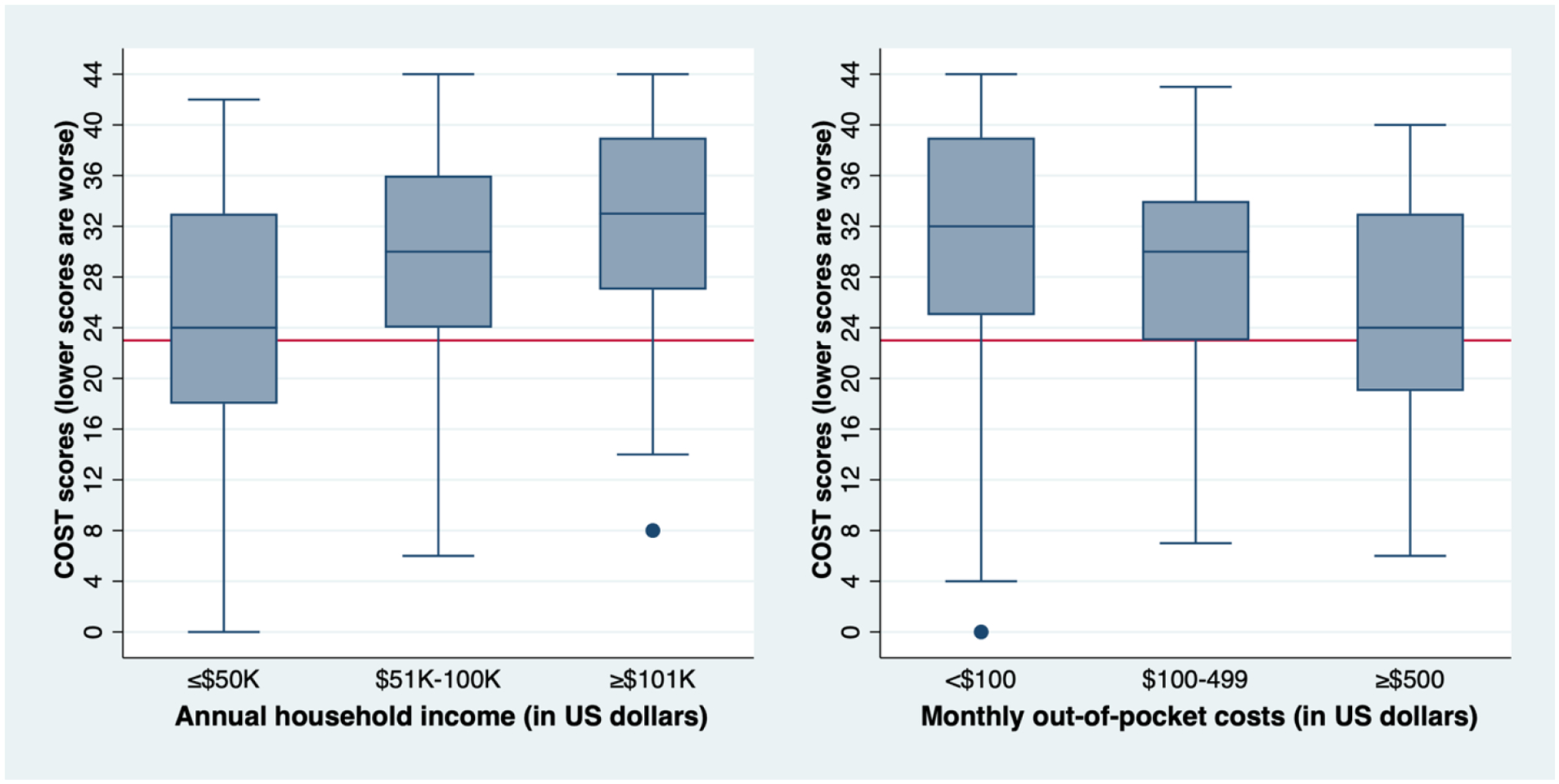
We conducted a single-center cross-sectional survey of patients with MM who had undergone transplantation. FinTox+ was defined as a COST-FACIT score <23, TimeTox+ as MM-related interactions (including phone calls) ≥1x weekly or ≥1x monthly in-person among far-residing patients, QOL using PROMIS Global Health, and functional status using patient-reported Karnofsky performance status (KPS).
Of 252 patients, 22% and 40% met FinTox+ and TimeTox+ criteria respectively. Respective FinTox+ and TimeTox+ proportions were 22%/37% for patients on maintenance, 22%/82% with active therapy, and 20%/14% with observation. FinTox+ predictors included annual income (P < .01) and out-of-pocket costs (P < .01). TimeTox+ predictors included disease status (P < .001), caregiver status (P = .01), far-residing status (P < .001), and out-of-pocket costs (P = .03). FinTox+ was associated with a clinically meaningful decrease in mental QOL, while TimeTox+ patients were more likely to have KPS ≤ 80.
In our large study, monetary status but not disease status predicted FinTox. Over a third of patients on maintenance reported TimeTox. FinTox+ was associated with decreased mental health, while TimeTox+ was associated with worse performance status. These two toxicities may negatively impact patient wellbeing, and studies of strategies to mitigate their impact are in development.
多发性骨髓瘤(MM)患者可能需要多年的治疗,这可能导致经济毒性(FinTox)或时间毒性(TimeTox)。在 MM 治疗的不同阶段,FinTox 和 TimeTox 的流行率、预测因素和生活质量(QOL)影响尚未得到描述。
我们对接受过移植的 MM 患者进行了一项单中心横断面调查。FinTox+定义为 COST-FACIT 评分<23,TimeTox+定义为远居患者每周至少 1 次 MM 相关电话或每月至少 1 次面对面交流,QOL 使用 PROMIS 全球健康,功能状态使用患者报告的卡诺夫斯基表现状态(KPS)。
在 252 名患者中,分别有 22%和 40%符合 FinTox+和 TimeTox+标准。分别有 22%/37%的维持治疗患者、22%/82%的有活性治疗患者和 20%/14%的观察患者符合 FinTox+和 TimeTox+标准。FinTox+的预测因素包括年收入(P<0.01)和自付费用(P<0.01)。TimeTox+的预测因素包括疾病状态(P<0.001)、照顾者状态(P=0.01)、远居状态(P<0.001)和自付费用(P=0.03)。FinTox+与心理健康的显著下降有关,而 TimeTox+患者更有可能出现 KPS≤80。
在我们的大型研究中,经济状况而非疾病状况预测了 FinTox。超过三分之一的维持治疗患者报告了 TimeTox。FinTox+与心理健康下降有关,而 TimeTox+与较差的表现状态有关。这两种毒性可能对患者的幸福感产生负面影响,目前正在研究减轻其影响的策略。