Fred Hutchinson Cancer Center, Seattle, WA, USA.
University of Washington, Seattle, WA, USA.
Blood Cancer J. 2024 Aug 27;14(1):149. doi: 10.1038/s41408-024-01129-0.
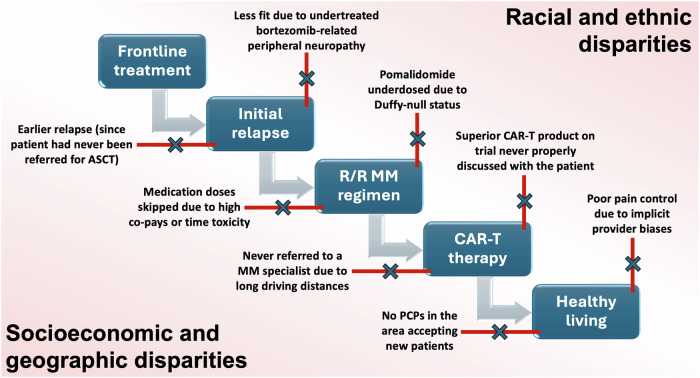
Many studies have documented racial, socioeconomic, geographic, and other disparities for United States (US) patients with multiple myeloma pertaining to diagnosis and frontline management. In contrast, very little is known about disparities in the management of relapsed/refractory multiple myeloma (RRMM) despite a plethora of novel treatment options. In this review, we discuss the manifestations of disparities in RRMM and strategies to mitigate their impact. Immunomodulatory drugs can create disparities on many axes, for example inappropriately low dosing due to Duffy-null status as well as time toxicity and financial toxicity from logistical hurdles for socioeconomically vulnerable patients. Access to myeloma expertise at high-volume centers is a critical consideration given the disconnect between how drugs like carfilzomib and dexamethasone are prescribed in trials versus optimized in real-world practice to lower toxicities. Disparities in chimeric antigen receptor T-cell therapy and bispecific antibody therapy span across racial, ethnic, and socioeconomic lines in large part due to their limited availability outside of high-volume centers. Another insidious source of disparities is supportive care in RRMM, ranging from inadequate pain control in Black patients to limited primary care provider access in rural settings. We discuss the rationales and evidence base for several solutions aimed at mitigating these disparities: for example, (1) bidirectional co-management with community-based oncologists, (2) screening for risk factors based on social determinants of health, (3) strategies to build patient trust with regard to clinical trials, and (4) longitudinal access to a primary care provider. As the treatment landscape for RRMM continues to expand, these types of efforts by the field will help ensure that this landscape is equally accessible and traversable for all US patients.
许多研究记录了美国(美国)多发性骨髓瘤患者在诊断和一线治疗方面存在种族、社会经济、地理和其他差异。相比之下,尽管有大量新的治疗选择,关于复发性/难治性多发性骨髓瘤(RRMM)管理方面的差异却知之甚少。在这篇综述中,我们讨论了 RRMM 管理中差异的表现形式以及减轻其影响的策略。免疫调节药物可能会在许多方面造成差异,例如由于 Duffy 阴性状态导致的剂量不当,以及对于社会经济弱势群体患者来说,由于后勤障碍导致的时间毒性和财务毒性。考虑到在临床试验中药物(如卡非佐米和地塞米松)的处方方式与在现实实践中优化以降低毒性之间存在脱节,在高容量中心获得骨髓瘤专业知识是一个关键因素。嵌合抗原受体 T 细胞疗法和双特异性抗体疗法的差异跨越了种族、民族和社会经济阶层,主要是由于它们在高容量中心之外的可用性有限。RRMM 支持性护理中的另一个潜在差异源是黑人患者的疼痛控制不足,以及农村地区基层医疗服务提供者的有限获取。我们讨论了旨在减轻这些差异的几种解决方案的理由和证据基础:例如,(1)与社区肿瘤学家双向共同管理,(2)根据健康的社会决定因素筛查风险因素,(3)建立临床试验患者信任的策略,以及(4)长期获得初级保健提供者。随着 RRMM 治疗领域的不断扩展,该领域的此类努力将有助于确保所有美国患者都能平等地获得和使用这一领域。