Department of Radiation Oncology, Division of Radiation Oncology, The University of Texas MD Anderson Cancer Center, Houston.
Department of Genitourinary Medical Oncology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, Houston.
JAMA Netw Open. 2024 Mar 4;7(3):e243379. doi: 10.1001/jamanetworkopen.2024.3379.
Subgroup analyses are often performed in oncology to investigate differential treatment effects and may even constitute the basis for regulatory approvals. Current understanding of the features, results, and quality of subgroup analyses is limited.
To evaluate forest plot interpretability and credibility of differential treatment effect claims among oncology trials.
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study included randomized phase 3 clinical oncology trials published prior to 2021. Trials were screened from ClinicalTrials.gov.
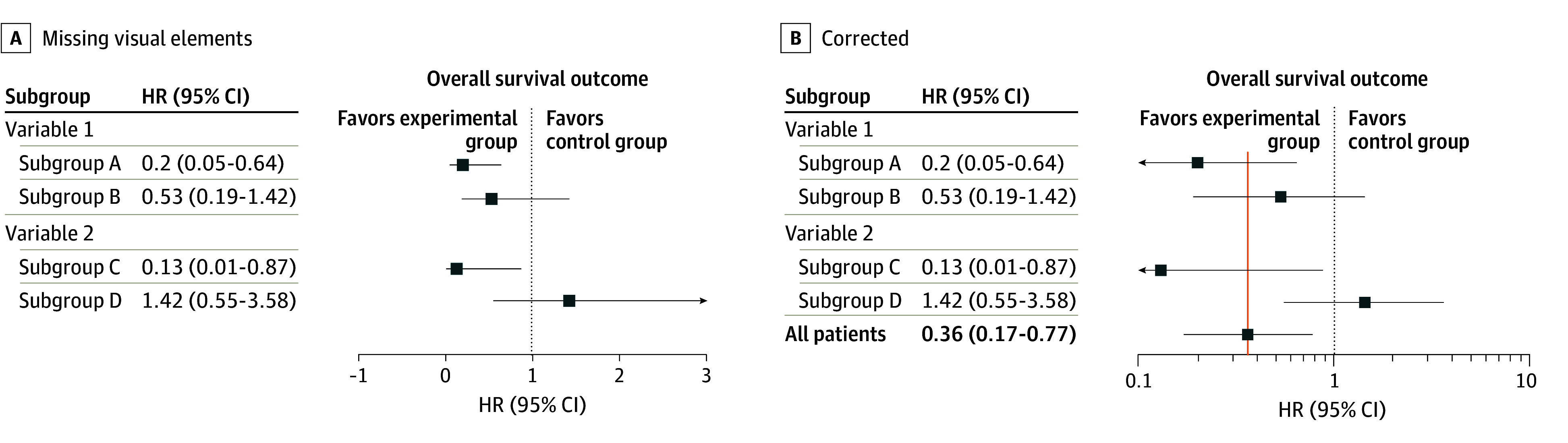
Missing visual elements in forest plots were defined as a missing point estimate or use of a linear x-axis scale for hazard and odds ratios. Multiplicity of testing control was recorded. Differential treatment effect claims were rated using the Instrument for Assessing the Credibility of Effect Modification Analyses. Linear and logistic regressions evaluated associations with outcomes.
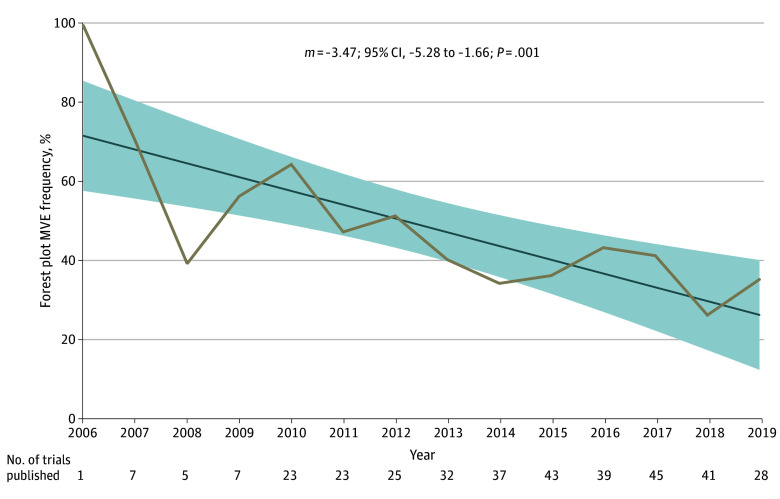
Among 785 trials, 379 studies (48%) enrolling 331 653 patients reported a subgroup analysis. The forest plots of 43% of trials (156 of 363) were missing visual elements impeding interpretability. While 4148 subgroup effects were evaluated, only 1 trial (0.3%) controlled for multiple testing. On average, trials that did not meet the primary end point conducted 2 more subgroup effect tests compared with trials meeting the primary end point (95% CI, 0.59-3.43 tests; P = .006). A total of 101 differential treatment effects were claimed across 15% of trials (55 of 379). Interaction testing was missing in 53% of trials (29 of 55) claiming differential treatment effects. Trials not meeting the primary end point were associated with greater odds of no interaction testing (odds ratio, 4.47; 95% CI, 1.42-15.55, P = .01). The credibility of differential treatment effect claims was rated as low or very low in 93% of cases (94 of 101).
In this cross-sectional study of phase 3 oncology trials, nearly half of trials presented a subgroup analysis in their primary publication. However, forest plots of these subgroup analyses largely lacked essential features for interpretation, and most differential treatment effect claims were not supported. Oncology subgroup analyses should be interpreted with caution, and improvements to the quality of subgroup analyses are needed.
在肿瘤学中,通常进行亚组分析以研究治疗效果的差异,甚至可能构成监管批准的基础。目前对亚组分析的特征、结果和质量的了解有限。
评估肿瘤学试验中差异治疗效果主张的森林图可解释性和可信度。
设计、地点和参与者:本横断面研究纳入了 2021 年前发表的随机 3 期临床肿瘤学试验。试验从 ClinicalTrials.gov 筛选。
森林图中缺失的可视元素定义为缺失点估计值或使用线性 x 轴比例来表示风险和优势比。记录了多重检验控制。使用评估效应修正分析可信度的工具对差异治疗效果主张进行评分。线性和逻辑回归评估了与结果的关联。
在 785 项试验中,379 项研究(48%)纳入了 331653 名患者,报告了亚组分析。43%(156/363)的试验森林图缺失了妨碍解释的可视元素。虽然评估了 4148 个亚组效应,但只有 1 项试验(0.3%)控制了多次检验。平均而言,未达到主要终点的试验比达到主要终点的试验多进行了 2 次亚组效果检验(95%CI,0.59-3.43 次;P=0.006)。共有 101 项差异治疗效果主张出现在 15%的试验中(55/379)。声称存在差异治疗效果的 55 项试验中有 53%(29/55)缺失交互检验。未达到主要终点的试验与交互检验缺失的可能性更大(比值比,4.47;95%CI,1.42-15.55,P=0.01)。93%(94/101)的差异治疗效果主张的可信度被评为低或极低。
在这项对 3 期肿瘤学试验的横断面研究中,近一半的试验在其主要出版物中呈现了亚组分析。然而,这些亚组分析的森林图在很大程度上缺乏解释的基本特征,并且大多数差异治疗效果主张都没有得到支持。肿瘤学亚组分析应谨慎解读,需要提高亚组分析的质量。