Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing), Department of Radiation Oncology, Peking University Cancer Hospital and Institute, 100142, Beijing, China.
BMC Geriatr. 2024 Apr 17;24(1):348. doi: 10.1186/s12877-024-04939-w.
Definitive chemoradiotherapy is one of the primary treatment modalities for older patients with esophageal cancer (EC). However, the evolution of prognosis over time and the factors affected non-EC deaths remain inadequately studied. We examined the conditional survival and annual hazard of death in older patients with EC after chemoradiotherapy.
We collected data from patients aged 65 or older with EC registered in the Surveillance, Epidemiology, and End Results database during 2000-2019. Conditional survival was defined as the probability of survival given a specific time survived. Annual hazard of death was defined the yearly event rate. Restricted cubic spline (RCS) analysis identified the association of age at diagnosis with mortality.
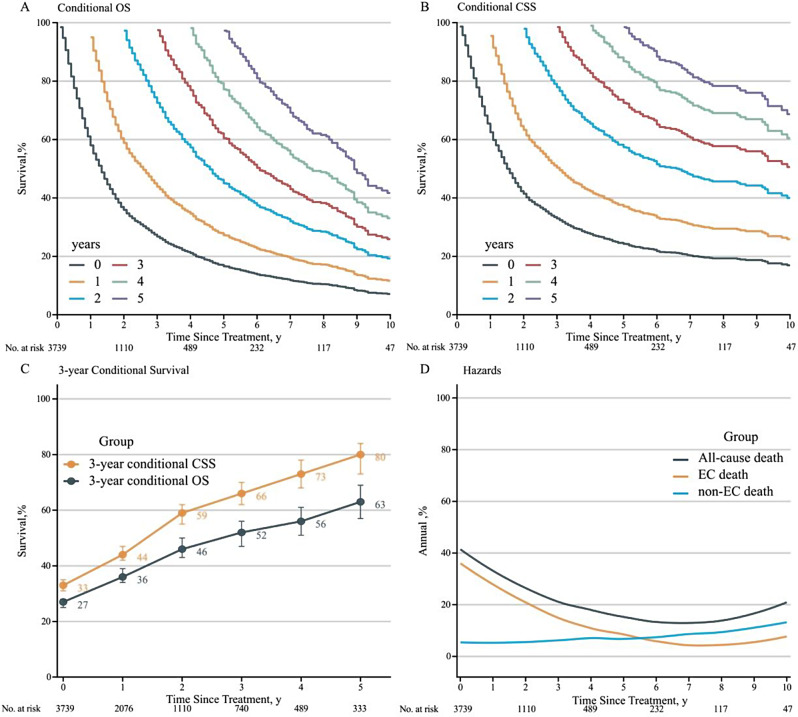
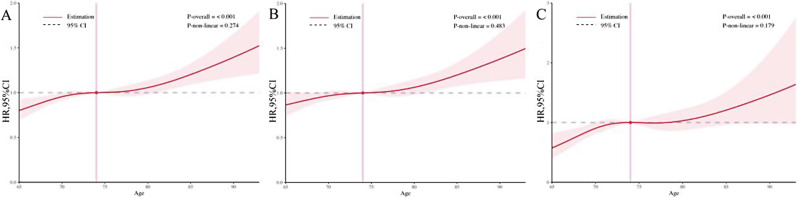
Among 3739 patients, the 3-year conditional overall survival increased annually by 7-10%. Non-EC causes accounted for 18.8% of deaths, predominantly due to cardio-cerebrovascular diseases. The hazard of death decreased from 40 to 10% in the first 6 years and then gradually increased to 20% in the tenth year. Non-EC causes surpassed EC causes in hazard starting 5 years post-treatment. RCS indicated a consistent increase in death hazard with advancing age, following a linear relationship. The overall cohort was divided into two groups: 65-74 and ≥ 75 years old, with the ≥ 75-year-old group showing poorer survival and earlier onset of non-EC deaths (HR = 1.36, 95% CI: 1.15-1.62, P < 0.001). Patients with early-stage disease (I-II) had higher risks of death from non-EC causes (HR = 0.82, 95% CI: 0.68-0.98, P = 0.035). Tumor histology had no significant impact on non-EC death risk (HR = 1.17, 95% CI: 0.98-1.39, P = 0.081).
Survival probability increases with time for older patients with EC treated with chemoradiotherapy. Clinicians and patients should prioritize managing and preventing age-related comorbidities, especially in older cohorts and those with early-stage disease.
放化疗是老年食管癌(EC)患者的主要治疗方式之一。然而,预后随时间的演变以及影响非 EC 死亡的因素尚未得到充分研究。我们研究了放化疗后老年 EC 患者的条件生存率和每年死亡风险。
我们从 2000 年至 2019 年在监测、流行病学和结果数据库中收集了年龄在 65 岁或以上的 EC 患者的数据。条件生存率定义为在特定生存时间内的生存概率。每年的死亡风险定义为每年的事件发生率。限制三次样条(RCS)分析确定了诊断时年龄与死亡率的关系。
在 3739 名患者中,3 年的条件总生存率每年增加 7-10%。非 EC 原因占死亡人数的 18.8%,主要是由于心脑血管疾病。死亡风险在前 6 年从 40%降至 10%,然后在第 10 年逐渐增加到 20%。非 EC 原因在治疗后 5 年内超过 EC 原因成为死亡的主要原因。RCS 显示,随着年龄的增长,死亡风险呈持续增加趋势,呈线性关系。整个队列分为两组:65-74 岁和≥75 岁,≥75 岁组的生存率较差,非 EC 死亡的发病时间更早(HR=1.36,95%CI:1.15-1.62,P<0.001)。早期疾病(I-II 期)患者死于非 EC 原因的风险更高(HR=0.82,95%CI:0.68-0.98,P=0.035)。肿瘤组织学对非 EC 死亡风险没有显著影响(HR=1.17,95%CI:0.98-1.39,P=0.081)。
接受放化疗的老年 EC 患者的生存概率随时间的推移而增加。临床医生和患者应优先管理和预防与年龄相关的合并症,尤其是在年龄较大的患者和早期疾病患者中。