Department of Gastrointestinal Surgery, The Affiliated Hospital of Qingdao University, 16# Jiangsu Road, Qingdao, Shandong Province, 266000, P.R. China.
World J Surg Oncol. 2024 Apr 17;22(1):101. doi: 10.1186/s12957-024-03348-y.
Although current guidelines(ESPEN guideline: Clinical nutrition in surgery and other guidelines) recommend preoperative immunonutrition for cachectic gastric cancer patients, the strength of the recommendation is weak, and the level of evidence is low. The benefits of preoperative immunonutrition still remain controversial.
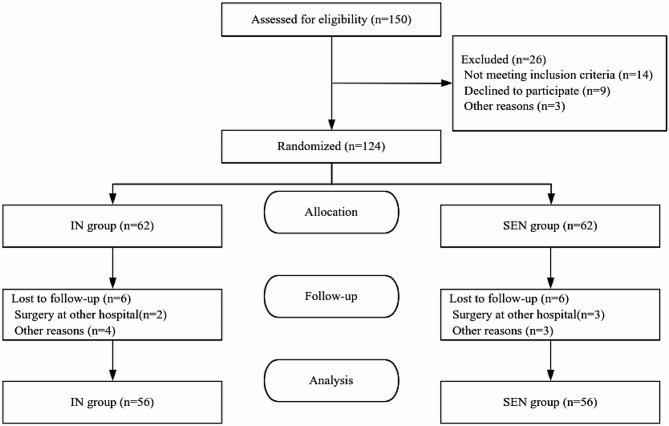
112 patients with gastric cancer cachexia were enrolled in the study and randomly assigned in a 1:1 ratio to receive either preoperative enteral immunonutrition support (IN, n = 56) or standard enteral nutrition support (SEN, n = 56). The primary endpoint was the incidence of infectious complications, and the secondary endpoints included the nutritional indicators, inflammatory markers, immune parameters, postoperative recovery and complications and gastrointestinal intolerance reactions.
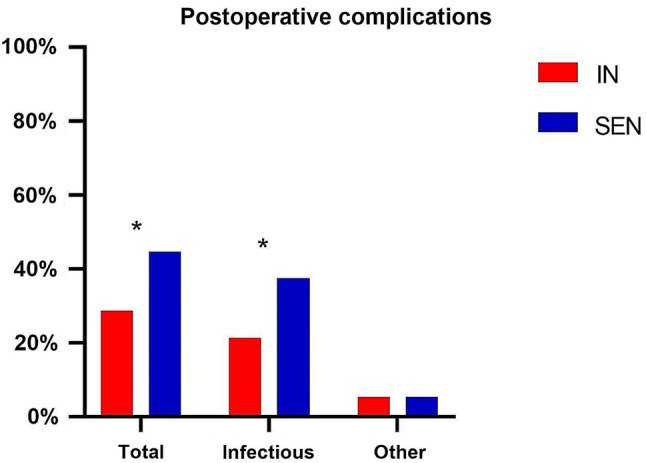
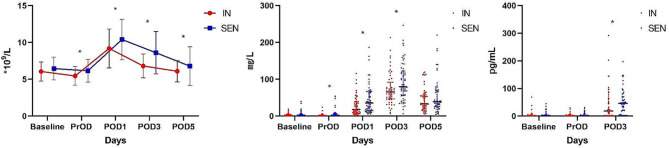
The incidence of postoperative infectious complications(P = 0.040) and overall complications (P = 0.049)was significantly lower in the IN group compared to the SEN group. In terms of laboratory inflammatory indexes, patients in the IN group demonstrated significantly lower levels of white blood cells (WBC), C-reactive protein (CRP), and interleukin-6 (IL-6), as well as higher levels of lymphocytes (LYMPH) and immunoglobulin A (IgA), compared to patients in the SEN group, with statistically significant differences. In terms of clinical outcomes, the IN group had a shorter duration of antibiotic use (P = 0.048), shorter hospital stay (P = 0.018), and lower total hospital costs (P = 0.034) compared to the SEN group. The IN group also experienced significantly less weight loss after surgery (P = 0.043).
Preoperative administration of immunonutrition formula has a positive impact on the incidence of infectious complications in patients with gastric cancer cachexia after surgery. It improves patients' inflammatory and immune status, shortens hospital stays, and reduces healthcare costs. Preoperative use of immunonutrition may contribute to the improvement of prognosis in this high-risk population.
尽管目前的指南(ESPEN 指南:手术中的临床营养和其他指南)建议对恶病质胃癌患者进行术前免疫营养,但推荐的强度较弱,证据水平较低。术前免疫营养的益处仍存在争议。
本研究纳入了 112 例胃癌恶病质患者,按照 1:1 的比例随机分为肠内免疫营养支持组(IN 组,n=56)和标准肠内营养支持组(SEN 组,n=56)。主要终点是感染性并发症的发生率,次要终点包括营养指标、炎症标志物、免疫参数、术后恢复和并发症以及胃肠道不耐受反应。
IN 组术后感染性并发症(P=0.040)和总并发症(P=0.049)的发生率明显低于 SEN 组。在实验室炎症指标方面,IN 组的白细胞(WBC)、C 反应蛋白(CRP)和白细胞介素-6(IL-6)水平明显低于 SEN 组,淋巴细胞(LYMPH)和免疫球蛋白 A(IgA)水平明显高于 SEN 组,差异有统计学意义。在临床结局方面,IN 组抗生素使用时间(P=0.048)、住院时间(P=0.018)和总住院费用(P=0.034)均明显短于 SEN 组。IN 组术后体重减轻也明显低于 SEN 组(P=0.043)。
术前给予免疫营养配方对胃癌恶病质患者术后感染性并发症的发生有积极影响。它改善了患者的炎症和免疫状态,缩短了住院时间,降低了医疗费用。术前使用免疫营养可能有助于改善这一高危人群的预后。