Translational Autoinflammatory Diseases Section, LCIM, NIAID, National Institutes of Health, Bethesda, Maryland, USA
Division of Pediatric Rheumatology, Children's Hospital of Pittsburgh of University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA.
Ann Rheum Dis. 2024 Aug 27;83(9):1181-1188. doi: 10.1136/ard-2023-225463.
Patients with chronic atypical neutrophilic dermatosis with lipodystrophy and elevated temperature/proteasome-associated autoinflammatory syndrome (CANDLE/PRAAS) respond to the janus kinase inhibitor 1/2 inhibition with baricitinib at exposures higher than in rheumatoid arthritis. Baricitinib dose reductions to minimise exposure triggered disease flares which we used to develop 'flare criteria'.
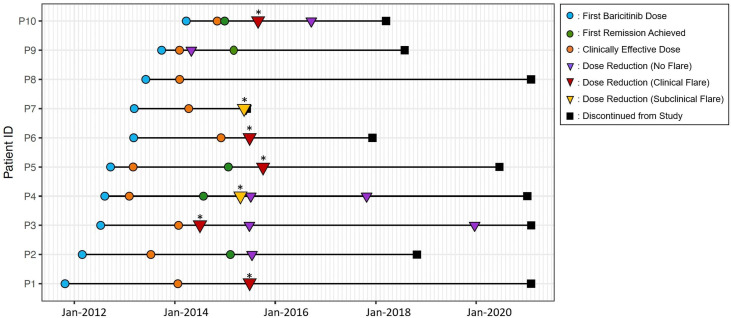
Of 10 patients with CANDLE/PRAAS treated with baricitinib in an open-label expanded-access programme, baricitinib doses were reduced 14 times in 9 patients between April 2014 and December 2019. Retrospective data analysis of daily diary scores and laboratory markers collected before and after the dose reductions were used to develop 'clinical' and 'subclinical' flare criteria. Disease flare rates were compared among patients with <25% and >25% dose reductions and during study visits when patients received recommended 'optimized' baricitinib doses (high-dose visits) versus lower than recommended baricitinib doses (low-dose visits) using two-sided χ tests.
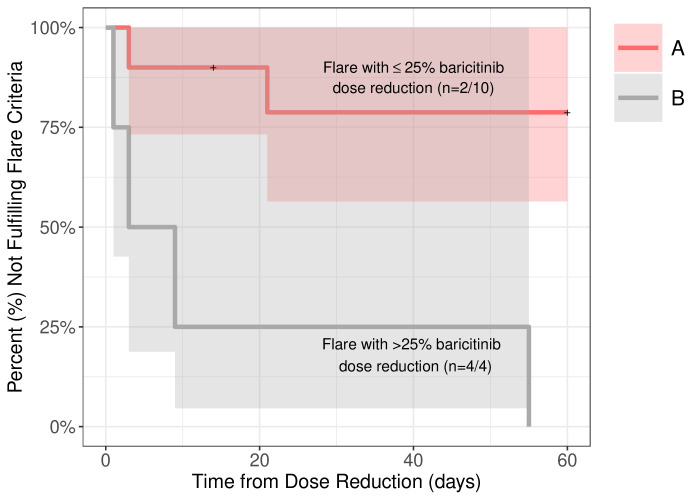
In the 9/10 patients with CANDLE with dose reduction, 7/14 (50%) times the dose was reduced resulted in a disease flare. All four dose reductions of >25% triggered a disease flare (p <0.05). Assessment of clinical and laboratory changes during disease flares allowed the development of disease flare criteria that were assessed during visits when patients received high or low doses of baricitinib. Disease flare criteria were reached during 43.14% of low-dose visits compared with 12.75% of high-dose visits (p <0.0001). Addition of an interferon score as an additional flare criterion increased the sensitivity to detect disease flares.
We observed disease flares and rebound inflammation with baricitinib dose reductions and proposed flare criteria that can assist in monitoring disease activity and in designing clinical studies in CANDLE/PRAAS.
患有慢性非典型中性粒细胞皮肤病伴脂肪营养不良和高温/蛋白酶体相关自身炎症综合征(CANDLE/PRAAS)的患者对 Janus 激酶抑制剂 1/2 抑制剂巴利昔替尼的反应是在高于类风湿关节炎的暴露水平下进行的。我们使用降低巴利昔替尼剂量以最小化暴露触发疾病发作的方法来开发“发作标准”。
在一项开放标签的扩展准入计划中,有 10 名 CANDLE/PRAAS 患者接受了巴利昔替尼治疗,其中 9 名患者在 2014 年 4 月至 2019 年 12 月期间 14 次减少了巴利昔替尼的剂量。对剂量减少前后收集的每日日记评分和实验室标志物的回顾性数据分析用于开发“临床”和“亚临床”发作标准。使用双侧 χ 检验比较患者中<25%和>25%剂量减少以及在接受推荐“优化”巴利昔替尼剂量(高剂量就诊)与低于推荐巴利昔替尼剂量(低剂量就诊)的研究就诊时的疾病发作率。
在 9/10 名接受 CANDLE 剂量减少的患者中,7/14(50%)次剂量减少导致疾病发作。所有 4 次>25%的剂量减少均触发疾病发作(p<0.05)。评估疾病发作期间的临床和实验室变化,允许开发疾病发作标准,这些标准在患者接受高或低剂量巴利昔替尼时的就诊期间进行评估。与高剂量就诊时的 12.75%相比,低剂量就诊时达到疾病发作标准的比例为 43.14%(p<0.0001)。添加干扰素评分作为附加的发作标准可提高检测疾病发作的敏感性。
我们观察到巴利昔替尼剂量减少与疾病发作和反弹炎症有关,并提出了发作标准,可用于监测疾病活动并设计 CANDLE/PRAAS 的临床研究。