Translational Autoinflammatory Disease Section, National Institute of Allergy and Infectious Diseases (NIAID), NIH, Bethesda, Maryland, USA.
Faculty of Physicians of the University of Nebraska Medical Center, College of Medicine, Omaha, Nebraska, USA.
J Clin Invest. 2018 Jul 2;128(7):3041-3052. doi: 10.1172/JCI98814. Epub 2018 Jun 11.
Monogenic IFN-mediated autoinflammatory diseases present in infancy with systemic inflammation, an IFN response gene signature, inflammatory organ damage, and high mortality. We used the JAK inhibitor baricitinib, with IFN-blocking activity in vitro, to ameliorate disease.
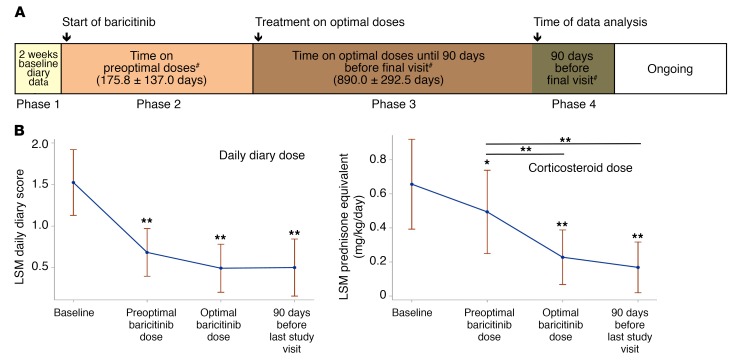
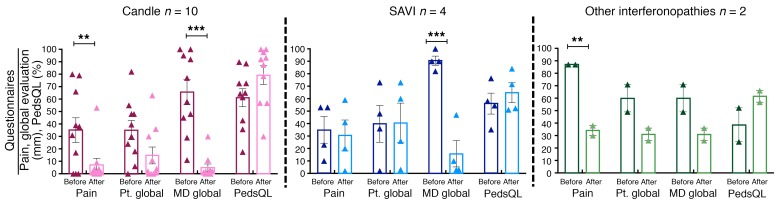
Between October 2011 and February 2017, 10 patients with CANDLE (chronic atypical neutrophilic dermatosis with lipodystrophy and elevated temperatures), 4 patients with SAVI (stimulator of IFN genes-associated [STING-associated] vasculopathy with onset in infancy), and 4 patients with other interferonopathies were enrolled in an expanded access program. The patients underwent dose escalation, and the benefit was assessed by reductions in daily disease symptoms and corticosteroid requirement. Quality of life, organ inflammation, changes in IFN-induced biomarkers, and safety were longitudinally assessed.
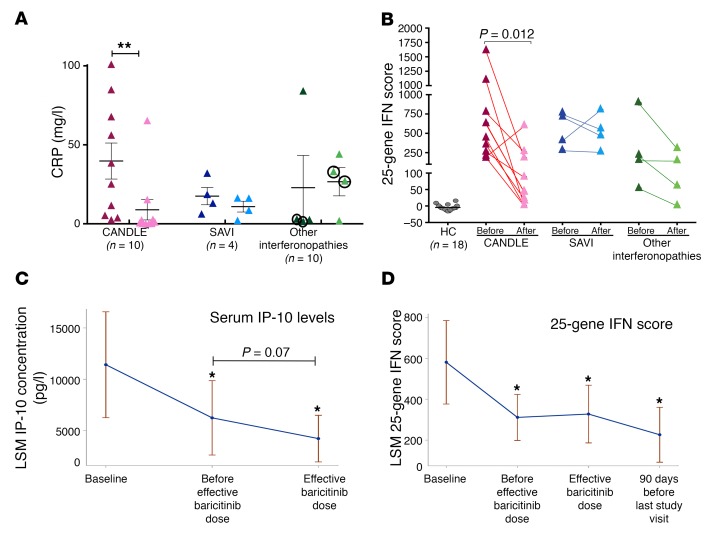
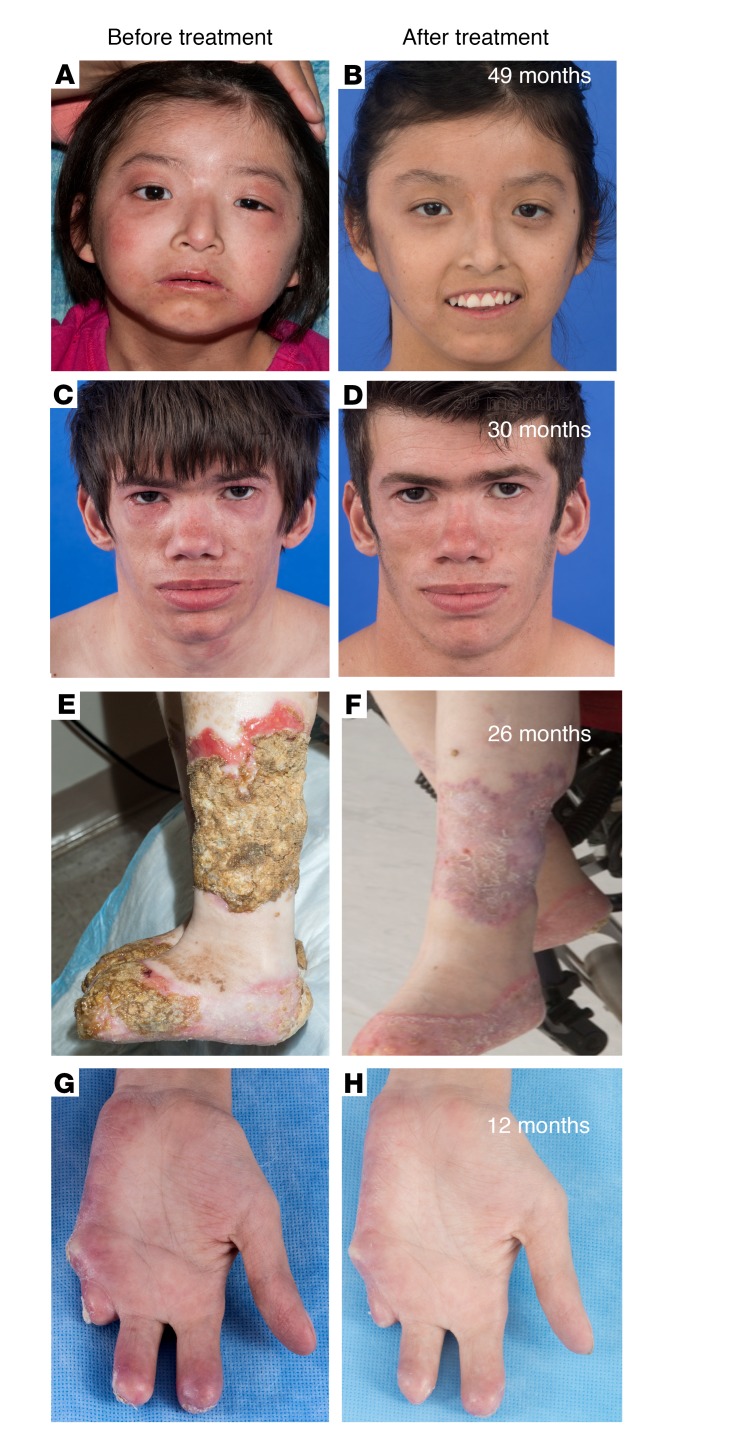
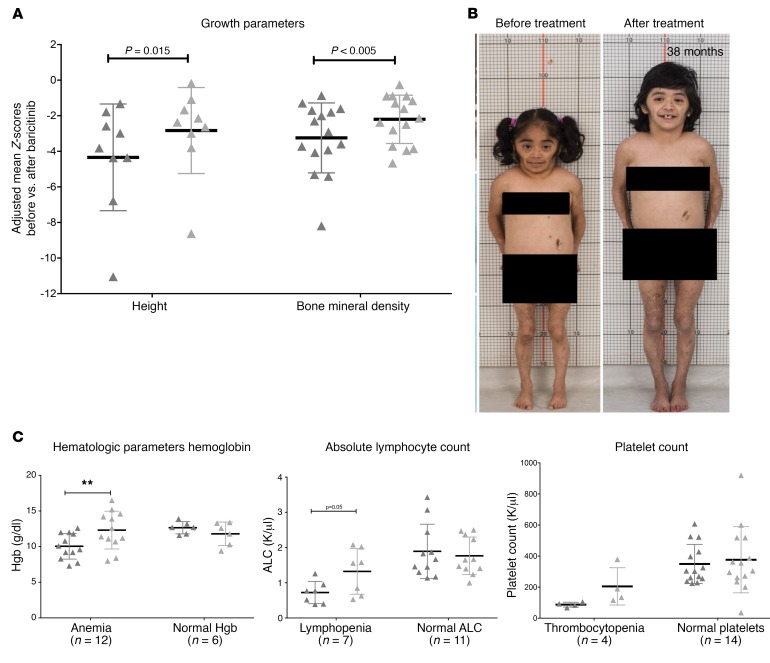
Eighteen patients were treated for a mean duration of 3.0 years (1.5-4.9 years). The median daily symptom score decreased from 1.3 (interquartile range [IQR], 0.93-1.78) to 0.25 (IQR, 0.1-0.63) (P < 0.0001). In 14 patients receiving corticosteroids at baseline, daily prednisone doses decreased from 0.44 mg/kg/day (IQR, 0.31-1.09) to 0.11 mg/kg/day (IQR, 0.02-0.24) (P < 0.01), and 5 of 10 patients with CANDLE achieved lasting clinical remission. The patients' quality of life and height and bone mineral density Z-scores significantly improved, and their IFN biomarkers decreased. Three patients, two of whom had genetically undefined conditions, discontinued treatment because of lack of efficacy, and one CANDLE patient discontinued treatment because of BK viremia and azotemia. The most common adverse events were upper respiratory infections, gastroenteritis, and BK viruria and viremia.
Upon baricitinib treatment, clinical manifestations and inflammatory and IFN biomarkers improved in patients with the monogenic interferonopathies CANDLE, SAVI, and other interferonopathies. Monitoring safety and efficacy is important in benefit-risk assessment.
ClinicalTrials.gov NCT01724580 and NCT02974595.
This research was supported by the Intramural Research Program of the NIH, NIAID, and NIAMS. Baricitinib was provided by Eli Lilly and Company, which is the sponsor of the expanded access program for this drug.
单基因 IFN 介导的自身炎症性疾病在婴儿期表现为全身炎症、IFN 反应基因特征、炎症性器官损伤和高死亡率。我们使用具有体外 IFN 阻断活性的 JAK 抑制剂巴瑞替尼来改善疾病。
2011 年 10 月至 2017 年 2 月,纳入了 10 例 CANDLE(慢性非典型中性粒细胞皮肤病伴脂肪营养不良和发热)、4 例 SAVI(干扰素基因相关刺激物[STING 相关]血管病,发病于婴儿期)和 4 例其他干扰素病患者,参与扩展访问项目。患者进行了剂量递增,通过减少每日疾病症状和皮质类固醇的需求来评估疗效。纵向评估了生活质量、器官炎症、IFN 诱导生物标志物的变化和安全性。
18 例患者的中位治疗时间为 3.0 年(1.5-4.9 年)。每日症状评分中位数从 1.3(四分位距 [IQR],0.93-1.78)降至 0.25(IQR,0.1-0.63)(P<0.0001)。在基线时接受皮质类固醇治疗的 14 例患者中,每日泼尼松剂量从 0.44mg/kg/天(IQR,0.31-1.09)降至 0.11mg/kg/天(IQR,0.02-0.24)(P<0.01),10 例 CANDLE 患者中有 5 例获得了持久的临床缓解。患者的生活质量和身高及骨密度 Z 评分显著改善,IFN 生物标志物降低。3 例患者(其中 2 例遗传条件不明)因疗效不佳而停止治疗,1 例 CANDLE 患者因 BK 病毒血症和氮质血症而停止治疗。最常见的不良事件是上呼吸道感染、胃肠炎和 BK 尿病毒血症和病毒血症。
在巴瑞替尼治疗后,CANDLE、SAVI 和其他干扰素病患者的临床症状和炎症及 IFN 生物标志物均得到改善。监测安全性和疗效对评估获益风险很重要。
ClinicalTrials.gov NCT01724580 和 NCT02974595。
本研究由美国国立卫生研究院(NIH)、国家过敏和传染病研究所(NIAID)和国家关节炎、肌肉骨骼和皮肤病研究所(NIAMS)的内部研究计划提供支持。巴瑞替尼由礼来公司提供,该公司是该药扩展访问计划的赞助商。