Farbu Bjørn Hoftun, Lydersen Stian, Mohus Randi Marie, Ueland Thor, Mollnes Tom Eirik, Klepstad Pål, Langeland Halvor
Department of Anaesthesiology and Intensive Care Medicine, St. Olav's University Hospital Trondheim, Norway.
Institute of Circulation and Medical Imaging, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology (NTNU), Trondheim, Norway.
Resusc Plus. 2024 Apr 17;18:100639. doi: 10.1016/j.resplu.2024.100639. eCollection 2024 Jun.
Ischaemic intestines could be a driver of critical illness through an inflammatory response. We have previously published reports on a biomarker for intestinal injury, plasma Intestinal Fatty Acid Binding Protein (IFABP), and inflammatory biomarkers after out-of-hospital cardiac arrest (OHCA). In this post-hoc study we explored the potential indirect effects of intestinal injury mediated through the inflammatory response on organ dysfunction and mortality.
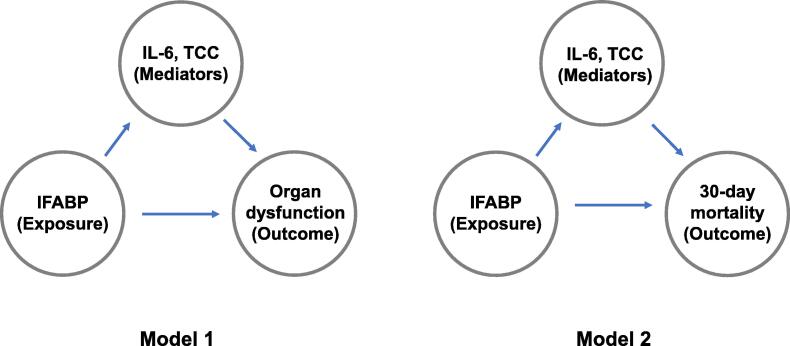
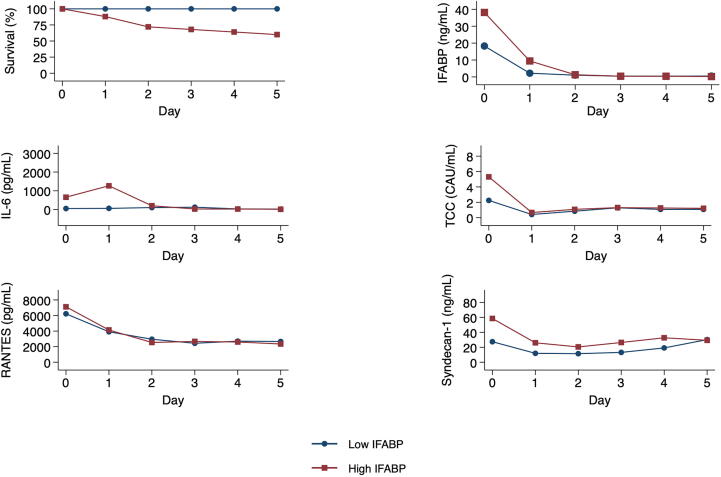
We measured IFABP and twenty-one inflammatory biomarkers in 50 patients at admission to intensive care unit after OHCA. First, we stratified patients on median IFABP and compared biomarkers between "low" and "high" IFABP. Second, by causal mediation analysis, we assessed effects of IFABP through the two most important inflammatory biomarkers, interleukin (IL)-6 and terminal complement complex (TCC), on day two circulatory variables, Sequential Organ Failure Assessment (SOFA)-score, and 30-day mortality.
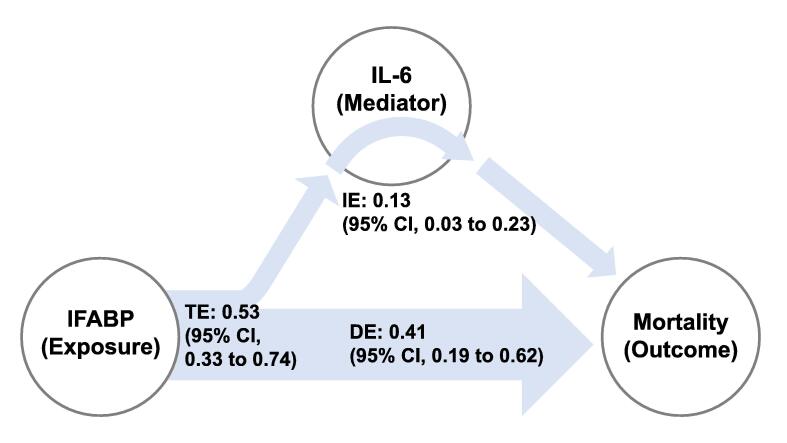
Cytokines and complement activation were higher in the high IFABP group. In mediation analysis, patients on the 75th percentile of IFABP, compared to the 25th percentile, had 53% (95% CI, 33-74; < 0.001) higher risk of dying, where 13 (95% CI, 3-23; = 0.01) percentage points were mediated through an indirect effect of IL-6. Similarly, the indirect effect of IFABP through IL-6 on SOFA-score was significant, but smaller than potential other effects. Effects through IL-6 on circulatory variables, and all effects through TCC, were not statistically significant and/or small.
Effects of intestinal injury mediated through inflammation on organ dysfunction and mortality were limited. Small, but significant, effects through IL-6 were noted.: ClinicalTrials.gov: NCT02648061.
缺血性肠病可能通过炎症反应成为危重病的驱动因素。我们之前已发表关于肠损伤生物标志物、血浆肠脂肪酸结合蛋白(IFABP)以及院外心脏骤停(OHCA)后炎症生物标志物的报告。在这项事后分析研究中,我们探讨了通过炎症反应介导的肠损伤对器官功能障碍和死亡率的潜在间接影响。
我们在50例OHCA后入住重症监护病房的患者入院时测量了IFABP和21种炎症生物标志物。首先,我们根据IFABP中位数对患者进行分层,并比较“低”IFABP组和“高”IFABP组之间的生物标志物。其次,通过因果中介分析,我们评估了IFABP通过两种最重要的炎症生物标志物白细胞介素(IL)-6和末端补体复合物(TCC)对第2天循环变量、序贯器官衰竭评估(SOFA)评分和30天死亡率的影响。
高IFABP组的细胞因子和补体激活水平更高。在中介分析中,与第25百分位数相比,处于IFABP第75百分位数的患者死亡风险高53%(95%CI,33 - 74;<0.001),其中13个百分点(95%CI,3 - 23;=0.01)是通过IL-6的间接作用介导的。同样,IFABP通过IL-6对SOFA评分的间接作用显著,但小于潜在的其他作用。通过IL-6对循环变量的作用以及通过TCC的所有作用均无统计学意义和/或作用较小。
炎症介导的肠损伤对器官功能障碍和死亡率的影响有限。通过IL-6观察到了较小但显著的影响。:ClinicalTrials.gov:NCT02648061。