Mayerhöfer Timo, Perschinka Fabian, Joannidis Michael
Gemeinsame Einrichtung für Intensiv- und Notfallmedizin, Department für Innere Medizin, Medizinische Universität Innsbruck, Innsbruck, Österreich.
Gemeinsame Einrichtung für Intensiv- und Notfallmedizin, Department für Innere Medizin, Medizinische Universität Innsbruck, Anichstr. 35, 6020, Innsbruck, Österreich.
Med Klin Intensivmed Notfmed. 2024 Jun;119(5):339-345. doi: 10.1007/s00063-024-01142-y. Epub 2024 Apr 29.
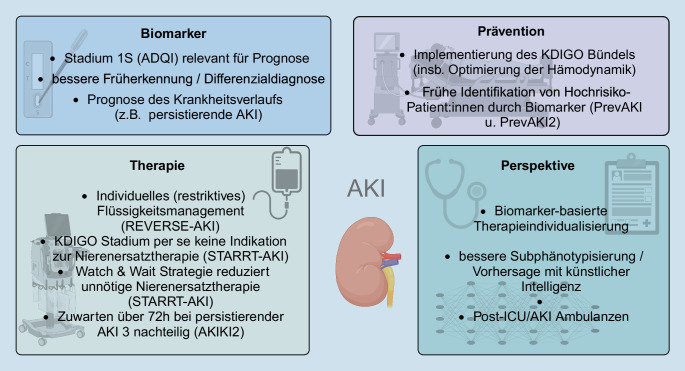
Acute kidney injury (AKI) is a common problem in critically ill patients and is associated with increased morbidity and mortality. Since 2012, AKI has been defined according to the KDIGO (Kidney Disease Improving Global Outcome) guidelines. As some biomarkers are now available that can provide useful clinical information, a new definition including a new stage 1S has been proposed by an expert group of the Acute Disease Quality Initiative (ADQI). At this stage, classic AKI criteria are not yet met, but biomarkers are already positive defining subclinical AKI. This stage 1S is associated with a worse patient outcome, regardless of the biomarker chosen. The PrevAKI and PrevAKI-Multicenter trial also showed that risk stratification with a biomarker and implementation of the KDIGO bundle (in the high-risk group) can reduce the rate of moderate and severe AKI. In the absence of a successful clinical trial, conservative management remains the primary focus of treatment. This mainly involves optimization of hemodynamics and an individualized (restrictive) fluid management. The STARRT-AKI trial has shown that there is no benefit from accelerated initiation of renal replacement therapy. However, delaying too long might be associated with potential harm, as shown in the AKIKI2 study. Prospective studies are needed to determine whether artificial intelligence will play a role in AKI in the future, helping to guide treatment decisions and improve outcomes.
急性肾损伤(AKI)是危重症患者的常见问题,与发病率和死亡率增加相关。自2012年以来,AKI一直根据KDIGO(改善全球肾脏病预后组织)指南进行定义。由于现在有一些生物标志物可提供有用的临床信息,急性疾病质量倡议(ADQI)专家组提出了一个新定义,包括一个新的1S期。在此阶段,尚未达到经典的AKI标准,但生物标志物已呈阳性,定义为亚临床AKI。无论选择何种生物标志物,这个1S期都与更差的患者预后相关。PrevAKI和PrevAKI多中心试验还表明,使用生物标志物进行风险分层并实施KDIGO综合治疗方案(在高危组)可降低中重度AKI的发生率。在缺乏成功临床试验的情况下,保守治疗仍然是主要的治疗重点。这主要包括优化血流动力学和个体化(限制性)液体管理。STARRT-AKI试验表明,加速启动肾脏替代治疗并无益处。然而,如AKIKI2研究所示,延迟时间过长可能会带来潜在危害。需要进行前瞻性研究以确定人工智能未来是否会在AKI中发挥作用,帮助指导治疗决策并改善预后。