Girardis Massimo, Coloretti Irene, Antonelli Massimo, Berlot Giorgio, Busani Stefano, Cortegiani Andrea, De Pascale Gennaro, De Rosa Francesco Giuseppe, De Rosa Silvia, Donadello Katia, Donati Abele, Forfori Francesco, Giannella Maddalena, Grasselli Giacomo, Montrucchio Giorgia, Oliva Alessandra, Pasero Daniela, Piazza Ornella, Romagnoli Stefano, Tascini Carlo, Viaggi Bruno, Tumbarello Mario, Viale Pierluigi
Anesthesia and Intensive Care Medicine, Policlinico Di Modena, University of Modena and Reggio Emilia, Modena, Italy.
Dipartimento Di Scienze Biotecnologiche Di Base, Cliniche Intensivologiche E Perioperatorie, Università Cattolica del Sacro Cuore, Rome, Italy.
J Anesth Analg Crit Care. 2024 Apr 30;4(1):28. doi: 10.1186/s44158-024-00165-3.
In the last decades, several adjunctive treatments have been proposed to reduce mortality in septic shock patients. Unfortunately, mortality due to sepsis and septic shock remains elevated and NO trials evaluating adjunctive therapies were able to demonstrate any clear benefit. In light of the lack of evidence and conflicting results from previous studies, in this multidisciplinary consensus, the authors considered the rational, recent investigations and potential clinical benefits of targeted adjunctive therapies.
A panel of multidisciplinary experts defined clinical phenotypes, treatments and outcomes of greater interest in the field of adjunctive therapies for sepsis and septic shock. After an extensive systematic literature review, the appropriateness of each treatment for each clinical phenotype was determined using the modified RAND/UCLA appropriateness method.
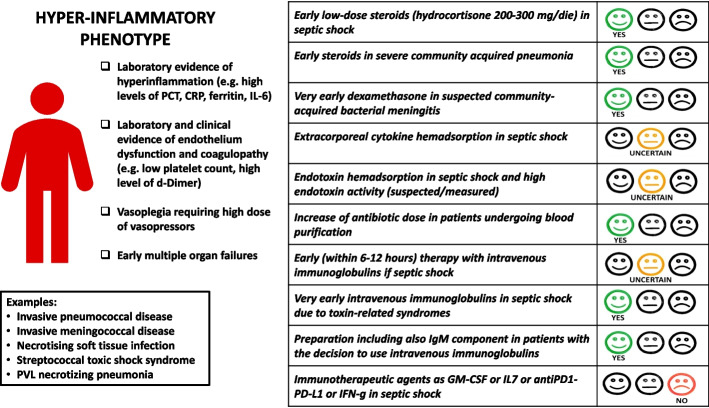
The consensus identified two distinct clinical phenotypes: patients with overwhelming shock and patients with immune paralysis. Six different adjunctive treatments were considered the most frequently used and promising: (i) corticosteroids, (ii) blood purification, (iii) immunoglobulins, (iv) granulocyte/monocyte colony-stimulating factor and (v) specific immune therapy (i.e. interferon-gamma, IL7 and AntiPD1). Agreement was achieved in 70% of the 25 clinical questions.
Although clinical evidence is lacking, adjunctive therapies are often employed in the treatment of sepsis. To address this gap in knowledge, a panel of national experts has provided a structured consensus on the appropriate use of these treatments in clinical practice.
在过去几十年中,已提出多种辅助治疗方法以降低脓毒症休克患者的死亡率。遗憾的是,脓毒症和脓毒症休克导致的死亡率仍然居高不下,且没有评估辅助治疗的试验能够证明有任何明显益处。鉴于缺乏证据以及先前研究结果相互矛盾,在本多学科共识中,作者考虑了靶向辅助治疗的合理性、近期研究及潜在临床益处。
一个多学科专家小组确定了脓毒症和脓毒症休克辅助治疗领域中更受关注的临床表型、治疗方法及结果。在广泛的系统文献综述之后,使用改良的兰德/加州大学洛杉矶分校适宜性方法确定每种治疗方法对每种临床表型的适宜性。
该共识确定了两种不同的临床表型:暴发性休克患者和免疫麻痹患者。六种不同的辅助治疗方法被认为是最常用且最有前景的:(i)皮质类固醇,(ii)血液净化,(iii)免疫球蛋白,(iv)粒细胞/单核细胞集落刺激因子,以及(v)特异性免疫治疗(即干扰素-γ、IL7和抗PD1)。在25个临床问题中有70%达成了共识。
尽管缺乏临床证据,但辅助治疗在脓毒症治疗中经常被采用。为填补这一知识空白,一个国家专家小组就这些治疗方法在临床实践中的合理使用达成了结构化共识。