Olds Anna, Gray W Hampton, Bojko Markian, Weaver Carly, Cleveland John D, Bowdish Michael E, Wells Winfield J, Starnes Vaughn A, Kumar S Ram
Division of Cardiac Surgery, Department of Surgery, Keck School of Medicine, University of Southern California, Los Angeles, Calif.
Division of Cardiac Surgery, Heart Institute, Children's Hospital of Los Angeles, Los Angeles, Calif.
JTCVS Open. 2024 Feb 17;18:180-192. doi: 10.1016/j.xjon.2024.02.006. eCollection 2024 Apr.
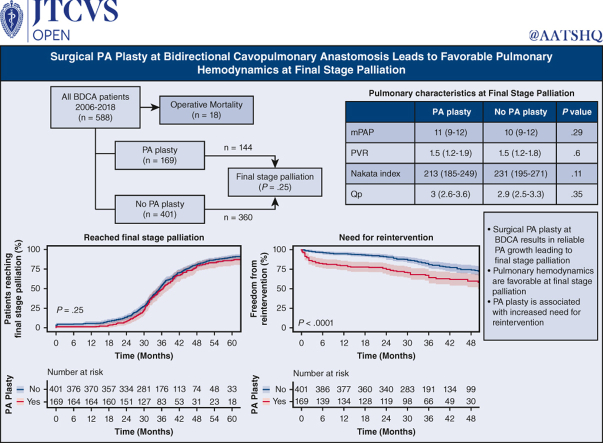
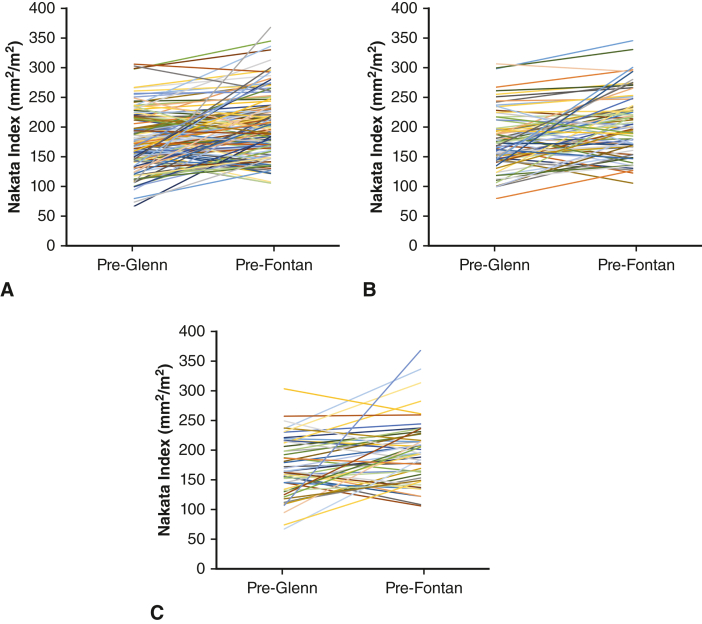
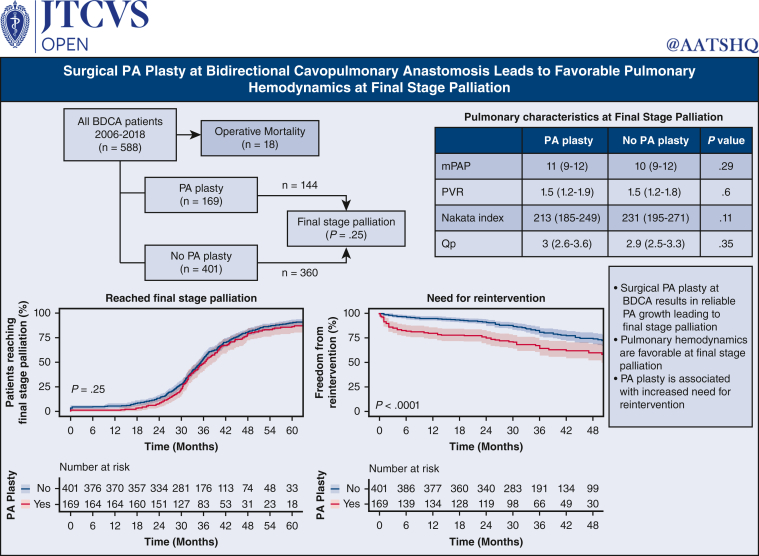
Pulmonary arterioplasty (PA plasty) at bidirectional cavopulmonary anastomosis (BDCA) is associated with increased morbidity, but outcomes to final stage palliation are unknown. We sought to determine the influence of PA plasty on pulmonary artery growth and hemodyamics at Fontan.
We retrospectively reviewed clinical data and outcomes for BDCA patients from 2006 to 2018. PA plasty was categorized by extent (type 1-4), as previously described. Outcomes included pulmonary artery reintervention and mortality before final palliation.
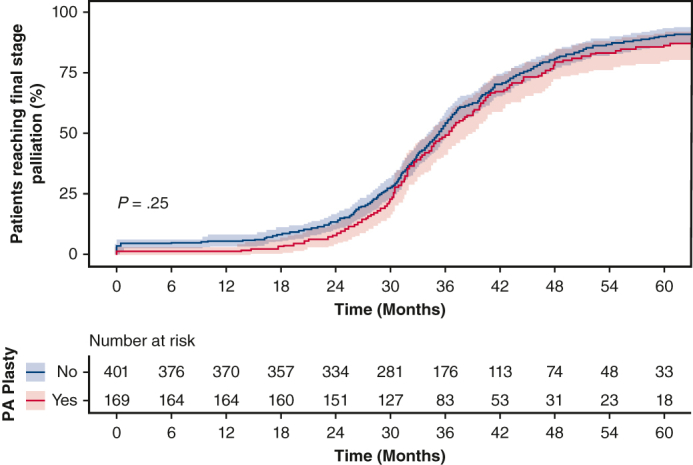
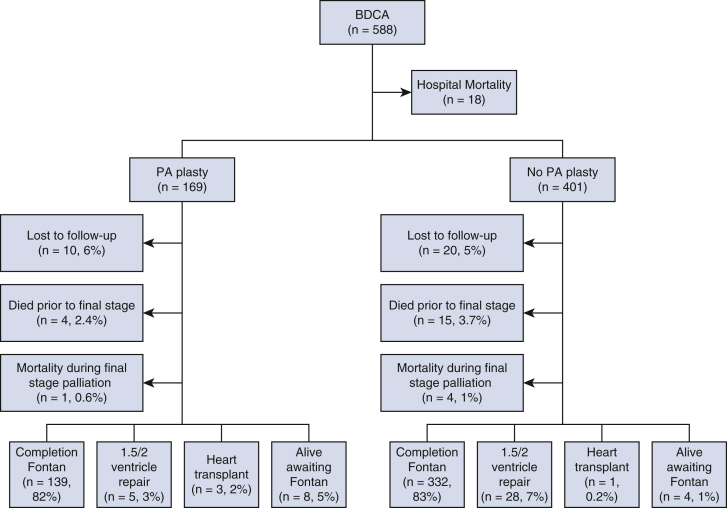
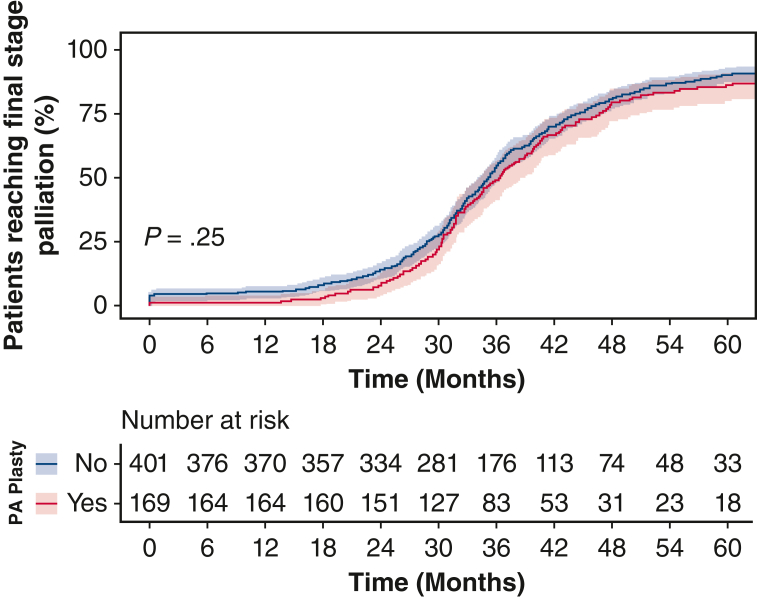
Five hundred eighty-eight patients underwent BDCA. One hundred seventy-nine patients (30.0%) underwent concomitant PA plasty. Five hundred seventy (97%) patients (169 [94%] PA plasty) survived to BDCA discharge. One hundred forty out of 570 survivors (25%) required PA/Glenn reintervention before final stage palliation (59 out of 169 [35%]) PA plasty; 81 out of 401 (20%) non-PA plasty; < .001). Twelve-, 24-, and 36-month freedom from reintervention after BDCA was 80% (95% CI, 74-86%), 75% (95% CI, 69-82%), and 64% (95% CI, 57-73%) for PA plasty, and 95% (95% CI, 93-97%), 91% (95% CI, 88-94%), and 81% (95% CI, 76-85%) for non-PA plasty ( < .001). Prefinal stage mortality was 37 (6.3%) (14 out of 169 PA plasty; 23 out of 401 non-PA plasty; = .4). Five hundred four (144 PA plasty and 360 non-PA plasty) patients reached final stage palliation (471 Fontan, 26 1.5-ventricle, and 7 2-ventricular repair). Pre-Fontan PA pressure and pulmonary vascular resistance were 10 mm Hg (range, 9-12 mm Hg) and 1.6 mm Hg (range, 1.3-1.9 mm Hg) in PA plasty and 10 mm Hg (range, 8-12 mm Hg) and 1.5 mm Hg (range, 1.3-1.9 mm Hg) in non-PA plasty patients, respectively ( = .29, .6). Fontan hospital mortality, length of stay, and morbidity were similar.
PA plasty at BDCA does not confer additional mortality risk leading to final palliation. Despite increased pulmonary artery reintervention, there was reliable pulmonary artery growth and favorable pulmonary hemodynamics at final stage palliation.
双向腔肺吻合术(BDCA)时行肺动脉成形术(PA成形术)与发病率增加相关,但至最终姑息治疗阶段的结局尚不清楚。我们旨在确定PA成形术对Fontan手术时肺动脉生长和血流动力学的影响。
我们回顾性分析了2006年至2018年BDCA患者的临床资料和结局。PA成形术按范围分类(1 - 4型),如前所述。结局包括最终姑息治疗前的肺动脉再次干预和死亡率。
588例患者接受了BDCA。179例患者(30.0%)同时接受了PA成形术。570例患者(97%)(169例[94%]PA成形术患者)存活至BDCA出院。570例幸存者中有140例(25%)在最终姑息治疗前需要进行PA/Glenn再次干预(169例PA成形术患者中有59例[35%];401例非PA成形术患者中有81例[20%];P<0.001)。BDCA后12个月、24个月和36个月无再次干预的比例,PA成形术患者分别为80%(95%CI,74 - 86%)、75%(95%CI,69 - 82%)和64%(95%CI,57 - 73%),非PA成形术患者分别为95%(95%CI,93 - 97%)、91%(95%CI,88 - 94%)和81%(95%CI,76 - 85%)(P<0.001)。最终姑息治疗前的死亡率为37例(6.3%)(169例PA成形术患者中有14例;401例非PA成形术患者中有23例;P = 0.4)。504例患者(144例PA成形术和360例非PA成形术)进入最终姑息治疗阶段(471例行Fontan手术,26例行1.5心室修复,7例行2心室修复)。Fontan手术前PA成形术患者的PA压力和肺血管阻力分别为10 mmHg(范围9 - 12 mmHg)和1.6 mmHg(范围1.3 - 1.9 mmHg),非PA成形术患者分别为10 mmHg(范围8 - 12 mmHg)和1.5 mmHg(范围1.3 - 1.9 mmHg)(P = 0.29,0.6)。Fontan手术的住院死亡率、住院时间和发病率相似。
BDCA时行PA成形术不会增加导致最终姑息治疗的额外死亡风险。尽管肺动脉再次干预增加,但在最终姑息治疗阶段肺动脉有可靠的生长且肺血流动力学良好。