Zhou Jiejie, Zhang Yang, Miao Haiwei, Yoon Ga Young, Wang Jinhao, Lin Yezhi, Wang Hailing, Liu Yan-Lin, Chen Jeon-Hor, Pan Zhifang, Su Min-Ying, Wang Meihao
Department of Radiology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, China.
Department of Radiological Sciences, University of California, Irvine, California, USA.
J Magn Reson Imaging. 2025 Feb;61(2):928-941. doi: 10.1002/jmri.29447. Epub 2024 May 10.
Accurate determination of human epidermal growth factor receptor 2 (HER2) is important for choosing optimal HER2 targeting treatment strategies. HER2-low is currently considered HER2-negative, but patients may be eligible to receive new anti-HER2 drug conjugates.
To use breast MRI BI-RADS features for classifying three HER2 levels, first to distinguish HER2-zero from HER2-low/positive (Task-1), and then to distinguish HER2-low from HER2-positive (Task-2).
Retrospective.
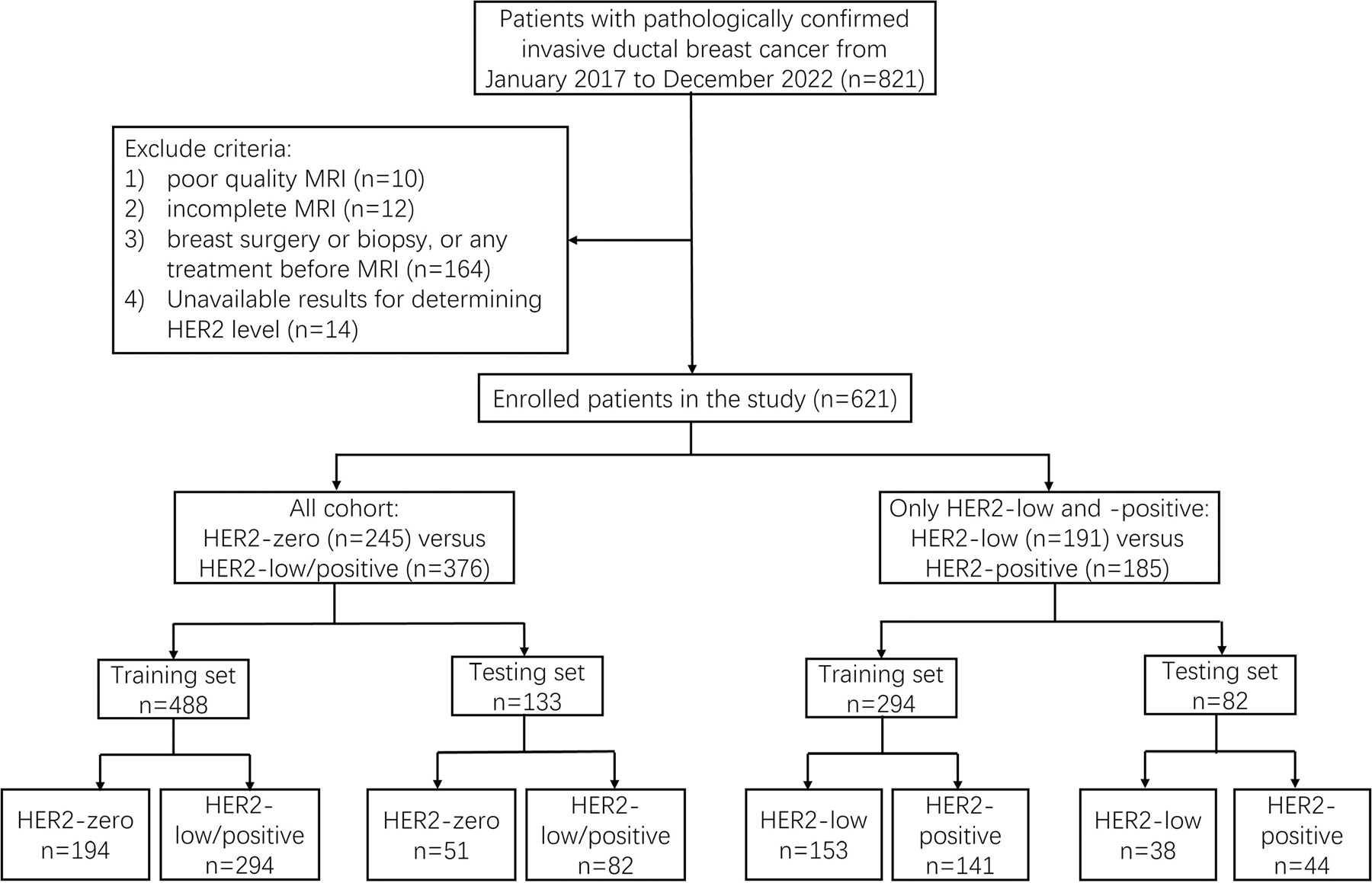
621 invasive ductal cancer, 245 HER2-zero, 191 HER2-low, and 185 HER2-positive. For Task-1, 488 cases for training and 133 for testing. For Task-2, 294 cases for training and 82 for testing.
FIELD STRENGTH/SEQUENCE: 3.0 T; 3D T1-weighted DCE, short time inversion recovery T2, and single-shot EPI DWI.
Pathological information and BI-RADS features were compared. Random Forest was used to select MRI features, and then four machine learning (ML) algorithms: decision tree (DT), support vector machine (SVM), k-nearest neighbors (k-NN), and artificial neural nets (ANN), were applied to build models.
Chi-square test, one-way analysis of variance, and Kruskal-Wallis test were performed. The P values <0.05 were considered statistically significant. For ML models, the generated probability was used to construct the ROC curves.
Peritumoral edema, the presence of multiple lesions and non-mass enhancement (NME) showed significant differences. For distinguishing HER2-zero from non-zero (low + positive), multiple lesions, edema, margin, and tumor size were selected, and the k-NN model achieved the highest AUC of 0.86 in the training set and 0.79 in the testing set. For differentiating HER2-low from HER2-positive, multiple lesions, edema, and margin were selected, and the DT model achieved the highest AUC of 0.79 in the training set and 0.69 in the testing set.
BI-RADS features read by radiologists from preoperative MRI can be analyzed using more sophisticated feature selection and ML algorithms to build models for the classification of HER2 status and identify HER2-low.
Stage 2.
准确测定人表皮生长因子受体2(HER2)对于选择最佳的HER2靶向治疗策略至关重要。HER2低表达目前被视为HER2阴性,但患者可能有资格接受新型抗HER2药物偶联物治疗。
利用乳腺MRI的BI-RADS特征对三种HER2水平进行分类,首先区分HER2零表达与HER2低表达/阳性(任务1),然后区分HER2低表达与HER2阳性(任务2)。
回顾性研究。
621例浸润性导管癌,245例HER2零表达,191例HER2低表达,185例HER2阳性。对于任务1,488例用于训练,133例用于测试。对于任务2,294例用于训练,82例用于测试。
场强/序列:3.0T;三维T1加权动态对比增强成像、短时间反转恢复T2加权成像和单次激发回波平面扩散加权成像。
比较病理信息和BI-RADS特征。使用随机森林选择MRI特征,然后应用四种机器学习(ML)算法:决策树(DT)、支持向量机(SVM)、k近邻(k-NN)和人工神经网络(ANN)构建模型。
进行卡方检验、单因素方差分析和Kruskal-Wallis检验。P值<0.05被认为具有统计学意义。对于ML模型,生成的概率用于构建ROC曲线。
瘤周水肿、多发病灶的存在和非肿块强化(NME)显示出显著差异。为了区分HER2零表达与非零表达(低表达+阳性),选择了多发病灶、水肿、边缘和肿瘤大小,k-NN模型在训练集中的AUC最高,为0.86,在测试集中为0.79。为了区分HER2低表达与HER2阳性,选择了多发病灶、水肿和边缘,DT模型在训练集中的AUC最高,为0.79,在测试集中为0.69。
放射科医生从术前MRI读取的BI-RADS特征可以通过更复杂的特征选择和ML算法进行分析,以构建HER2状态分类模型并识别HER2低表达。
2级。