Red Cross War Memorial Children's Hospital (RCWMCH), Rondebosch, Cape Town, South Africa.
University of Cape Town, Cape Town, South Africa.
Pediatr Nephrol. 2024 Sep;39(9):2807-2818. doi: 10.1007/s00467-024-06399-1. Epub 2024 May 11.
Dialysis is lifesaving for acute kidney injury (AKI), but access is poor in less resourced settings. A "peritoneal dialysis (PD) first" policy for paediatric AKI is more feasible than haemodialysis in low-resource settings.
Retrospective review of modalities and outcomes of children dialysed acutely at Red Cross War Memorial Children's Hospital between 1998 and 2020.
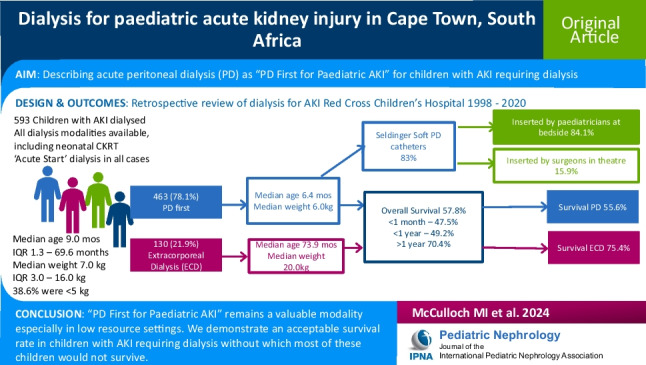
Of the 593 children with AKI who received dialysis, 463 (78.1%) received PD first. Median age was 9.0 (range 0.03-219.3; IQR 13.0-69.6) months; 57.6% were < 1 year old. Weights ranged from 0.9 to 2.0 kg (median 7.0 kg, IQR 3.0-16.0 kg); 38.6% were < 5 kg. PD was used more in younger children compared to extracorporeal dialysis (ECD), with median ages 6.4 (IQR 0.9-30.4) vs. 73.9 (IQR 17.5-113.9) months, respectively (p = 0.001). PD was performed with Seldinger soft catheters (n = 480/578, 83%), predominantly inserted by paediatricians at the bedside (n = 412/490, 84.1%). Complications occurred in 127/560 (22.7%) children receiving PD. Overall, 314/542 (57.8%) children survived. Survival was significantly lower in neonates (< 1 month old, 47.5%) and infants (1-12 months old, 49.2%) compared with older children (> 1 year old, 70.4%, p < 0.0001). Survival was superior in the ECD (75.4%) than in the PD group (55.6%, p = 0.002).
"PD First for Paediatric AKI" is a valuable therapeutic approach for children with AKI. It is feasible in low-resourced settings where bedside PD catheter insertion can be safely taught and is an acceptable dialysis modality, especially in settings where children with AKI would otherwise not survive.
透析是急性肾损伤(AKI)患者的救命疗法,但在资源较少的环境中,透析的可及性较差。对于资源较少的环境中的儿科 AKI 患者,“腹膜透析(PD)优先”策略比血液透析更可行。
回顾性分析 1998 年至 2020 年期间在红十字会纪念儿童医院接受急性透析的 593 例 AKI 患儿的治疗方式和结局。
在接受透析的 593 例 AKI 患儿中,463 例(78.1%)首先接受 PD 治疗。中位年龄为 9.0 岁(范围 0.03-219.3;IQR 13.0-69.6);57.6%的患儿年龄小于 1 岁。体重范围为 0.9-2.0kg(中位数为 7.0kg,IQR 3.0-16.0kg);38.6%的患儿体重小于 5kg。与体外透析(ECD)相比,PD 在更年幼的儿童中应用更为广泛,其中位年龄分别为 6.4(IQR 0.9-30.4)岁和 73.9(IQR 17.5-113.9)岁(p=0.001)。PD 使用 Seldinger 软导管进行(n=480/578,83%),主要由儿科医生在床边插入(n=412/490,84.1%)。在接受 PD 治疗的 127/560 名(22.7%)患儿中出现了并发症。总体而言,314/542 名(57.8%)患儿存活。与年龄较大的儿童(>1 岁,70.4%)相比,新生儿(<1 个月龄,47.5%)和婴儿(1-12 个月龄,49.2%)的存活率明显较低(p<0.0001)。与 PD 组(55.6%)相比,ECD 组(75.4%)的存活率更高(p=0.002)。
“PD 优先用于儿科 AKI”是治疗 AKI 患儿的一种有价值的治疗方法。在资源较少的环境中,床边 PD 导管插入术可以安全地教授,且是一种可接受的透析方式,尤其是在那些否则患儿将无法存活的环境中,这是一种可行的方法。