Department of Global Public Health, Karolinska Institutet, Stockholm, Sweden
Department of Community Medicine, University College Hospital, Ibadan, Nigeria.
BMJ Glob Health. 2024 May 16;9(5):e014902. doi: 10.1136/bmjgh-2023-014902.
Efforts to improve oxygen access have focused mainly on the supply side, but it is important to understand demand barriers, such as oxygen refusal among caregivers. We therefore aimed to understand caregiver, community and healthcare provider (HCP) perspectives and experiences of medical oxygen treatments and how these shape oxygen acceptance among caregivers of sick children in Lagos and Jigawa states, which are two contrasting settings in Nigeria.
Between April 2022 and January 2023, we conducted an exploratory qualitative study using reflexive thematic analysis, involving semistructured interviews with caregivers (Jigawa=18 and Lagos=7), HCPs (Jigawa=7 and Lagos=6) and community group discussions (Jigawa=4 and Lagos=5). We used an inductive-deductive approach to identify codes and themes through an iterative process using the theoretical framework of acceptability and the normalisation process theory as the analytic lens.
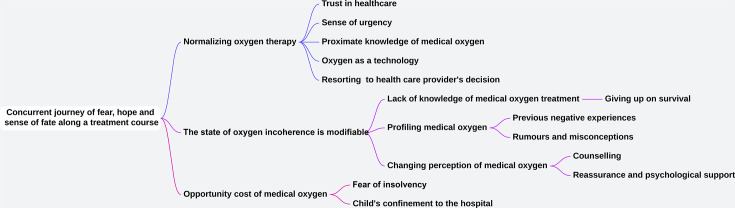
Medical oxygen prescription was associated with tension, characterised by fear of death, hopelessness about a child's survival and financial distress. These were driven by community narratives around oxygen, past negative experiences and contextual differences between both settings. Caregiver acceptance of medical oxygen was a sense-making process from apprehension and scepticism about their child's survival chances to positioning prescribed oxygen as an 'appropriate' or 'needed' intervention. Achieving this transition occurred through various means, such as trust in HCPs, a perceived sense of urgency for care, previous positive experience of oxygen use and a symbolic perception of oxygen as a technology. Misconceptions and pervasive negative narratives were acknowledged in Jigawa, while in Lagos, the cost was a major reason for oxygen refusal.
Non-acceptance of medical oxygen treatment for sick children is modifiable in the Nigerian context, with the root causes of refusal being contextually specific. Therefore, a one-size-fits-all policy is unlikely to work. Financial constraints and community attitudes should be addressed in addition to improving client-provider interactions.
为改善氧气获取而做出的努力主要集中在供应端,但了解需求障碍也很重要,例如照顾者拒绝使用氧气。因此,我们旨在了解照顾者、社区和医疗保健提供者(HCP)对医用氧气治疗的看法和经验,以及这些看法和经验如何影响拉各斯和吉加瓦州照顾者对患病儿童接受氧气治疗的态度,这两个州是尼日利亚两个截然不同的环境。
在 2022 年 4 月至 2023 年 1 月期间,我们进行了一项探索性定性研究,使用反思性主题分析方法,对照顾者(吉加瓦州=18 人,拉各斯州=7 人)、HCP(吉加瓦州=7 人,拉各斯州=6 人)和社区小组讨论(吉加瓦州=4 人,拉各斯州=5 人)进行半结构化访谈。我们使用了一种归纳演绎方法,通过理论框架(可接受性和正常化过程理论)的理论视角,通过迭代过程来识别代码和主题。
医用氧气处方与紧张有关,其特征是对孩子死亡的恐惧、对孩子生存的绝望和经济困境。这些紧张情绪是由社区围绕氧气的叙述、过去的负面经历以及两个环境之间的差异驱动的。照顾者对医用氧气的接受是一个从对孩子生存机会的疑虑和怀疑到将规定的氧气定位为“适当”或“需要”干预的意义建构过程。实现这种转变是通过各种方式实现的,例如对 HCP 的信任、对护理的紧迫感、以前使用氧气的积极经验以及将氧气视为一种技术的象征意义。在吉加瓦州,人们承认存在误解和普遍的负面叙述,而在拉各斯州,费用是拒绝使用氧气的主要原因。
在尼日利亚的背景下,对患病儿童的医用氧气治疗的非接受性是可以改变的,拒绝治疗的根本原因是具体的背景。因此,一刀切的政策不太可能奏效。除了改善医患互动外,还应解决财务限制和社区态度问题。