Mendoza-Hernandez Martha A, Hernandez-Fuentes Gustavo A, Sanchez-Ramirez Carmen A, Rojas-Larios Fabian, Guzman-Esquivel Jose, Rodriguez-Sanchez Iram P, Martinez-Fierro Margarita L, Cardenas-Rojas Martha I, De-Leon-Zaragoza Luis, Trujillo-Hernandez Benjamin, Fuentes-Murguia Mercedes, Ochoa-Díaz-López Héctor, Sánchez-Meza Karmina, Delgado-Enciso Ivan
Department of Molecular Medicine, School of Medicine, University of Colima, Colima 28040, Mexico.
COVID Unit, General Hospital Number 1, Mexican Institute of Social Security, Villa de Alvarez, Colima 28984, Mexico.
Biomed Rep. 2024 May 9;20(6):100. doi: 10.3892/br.2024.1788. eCollection 2024 Jun.
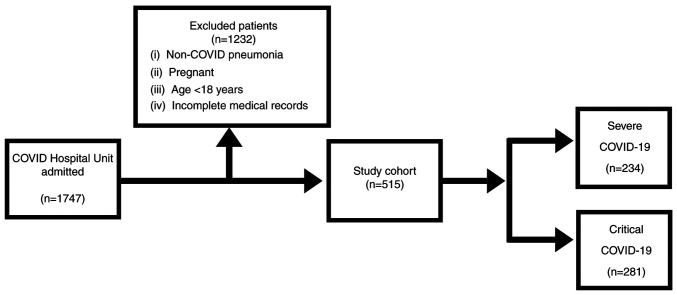
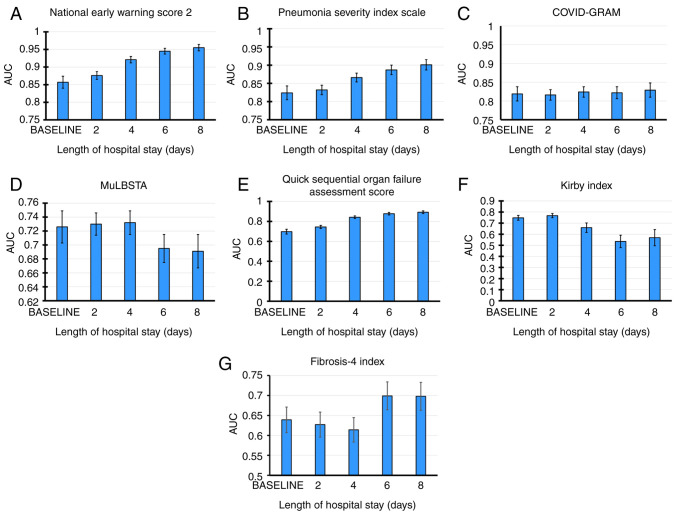
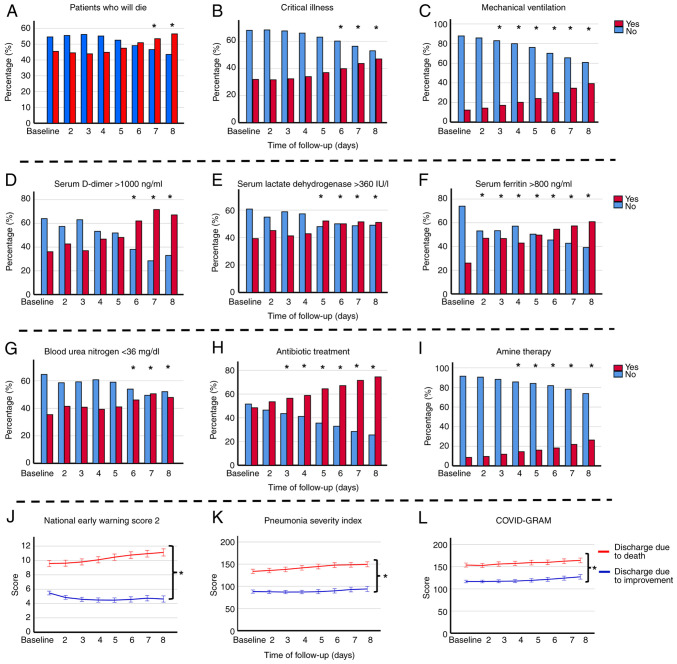
Clinical data from hospital admissions are typically utilized to determine the prognostic capacity of Coronavirus disease 2019 (COVID-19) indices. However, as disease status and severity markers evolve over time, time-dependent receiver operating characteristic (ROC) curve analysis becomes more appropriate. The present analysis assessed predictive power for death at various time points throughout patient hospitalization. In a cohort study involving 515 hospitalized patients (General Hospital Number 1 of Mexican Social Security Institute, Colima, Mexico from February 2021 to December 2022) with COVID-19, seven severity indices [Pneumonia Severity Index (PSI) PaO/FiO arterial oxygen pressure/fraction of inspired oxygen (Kirby index), the Critical Illness Risk Score (COVID-GRAM), the National Early Warning Score 2 (NEWS-2), the quick Sequential Organ Failure Assessment score (qSOFA), the Fibrosis-4 index (FIB-4) and the Viral Pneumonia Mortality Score (MuLBSTA were evaluated using time-dependent ROC curves. Clinical data were collected at admission and at 2, 4, 6 and 8 days into hospitalization. The study calculated the area under the curve (AUC), sensitivity, specificity, and predictive values for each index at these time points. Mortality was 43.9%. Throughout all time points, NEWS-2 demonstrated the highest predictive power for mortality, as indicated by its AUC values. PSI and COVID-GRAM followed, with predictive power increasing as hospitalization duration progressed. Additionally, NEWS-2 exhibited the highest sensitivity (>96% in all periods) but showed low specificity, which increased from 22.9% at admission to 58.1% by day 8. PSI displayed good predictive capacity from admission to day 6 and excellent predictive power at day 8 and its sensitivity remained >80% throughout all periods, with moderate specificity (70.6-77.3%). COVID-GRAM demonstrated good predictive capacity across all periods, with high sensitivity (84.2-87.3%) but low-to-moderate specificity (61.5-67.6%). The qSOFA index initially had poor predictive power upon admission but improved after 4 days. FIB-4 had a statistically significant predictive capacity in all periods (P=0.001), but with limited clinical value (AUC, 0.639-0.698), and with low sensitivity and specificity. MuLBSTA and IKIRBY exhibited low predictive power at admission and no power after 6 days. In conclusion, in COVID-19 patients with high mortality rates, NEWS-2 and PSI consistently exhibited predictive power for death during hospital stay, with PSI demonstrating the best balance between sensitivity and specificity.
医院住院患者的临床数据通常用于确定2019冠状病毒病(COVID-19)指标的预后能力。然而,随着疾病状态和严重程度标志物随时间演变,时间依赖型受试者工作特征(ROC)曲线分析变得更为合适。本分析评估了患者住院期间各个时间点的死亡预测能力。在一项队列研究中,纳入了515例住院的COVID-19患者(来自墨西哥社会保障局第一综合医院,墨西哥科利马,2021年2月至2022年12月),使用时间依赖型ROC曲线评估了七个严重程度指标[肺炎严重程度指数(PSI)、动脉血氧分压/吸入氧分数(Kirby指数)、危重病风险评分(COVID-GRAM)、国家早期预警评分2(NEWS-2)、快速序贯器官衰竭评估评分(qSOFA)、纤维化-4指数(FIB-4)和病毒性肺炎死亡率评分(MuLBSTA)]。在入院时以及住院第2、4、6和8天收集临床数据。该研究计算了这些时间点每个指标的曲线下面积(AUC)、敏感性、特异性和预测值。死亡率为43.9%。在所有时间点中,NEWS-2的AUC值表明其对死亡率的预测能力最高。PSI和COVID-GRAM次之,其预测能力随着住院时间的延长而增加。此外,NEWS-2的敏感性最高(在所有时期均>96%),但特异性较低,从入院时的22.9%增加到第8天时的58.1%。PSI从入院到第6天显示出良好的预测能力,在第8天具有出色的预测能力,并且其敏感性在所有时期均保持>80%,特异性中等(70.6-77.3%)。COVID-GRAM在所有时期均显示出良好的预测能力,敏感性高(84.2-87.3%),但特异性低至中等(61.5-67.6%)。qSOFA指数入院时预测能力较差,但4天后有所改善。FIB-4在所有时期均具有统计学显著的预测能力(P=0.001),但临床价值有限(AUC,0.639-0.698),且敏感性和特异性较低。MuLBSTA和Kirby指数入院时预测能力较低,6天后则无预测能力。总之,在死亡率较高的COVID-19患者中,NEWS-2和PSI在住院期间始终表现出对死亡的预测能力,其中PSI在敏感性和特异性之间表现出最佳平衡。